What is a Hernia?
What is a Hernia?
A hernia is a protrusion of the intestine through the muscle wall (typically in the region of the abdomen), creating a bulge in the skin. Hernias are more common than one may think, for males the lifetime risk is 27%. It can be painful or benign depending on the site in the body and size.
The probability of complications is greatest in the early stage so seek a medical diagnosis at the earliest possible stage even if your hernia seems asymptomatic (benign).
Hernias are classified as either single (unilateral) or double (bilateral) hernia. 54% will present to a doctor with a right-sided, 39.7% left-sided and 6.3% will be unlucky enough to have a bilateral hernia i.e. one either side of the groin.
How is a hernia caused?
Straining the area around a weak point of the abdomen can cause a hernia. Contributing factors for this are thought to be:
-
Obesity / poor diet.
-
Smokers cough or hard coughing generally.
-
Constipation.
-
Lifting or pushing heavy loads.
-
Weakening of the muscle wall as a result of age
-
Genetic predisposition.
Source
Demographic Profile
If you are aged 50+ and male you are more likely to have a hernia than the general population as a whole. This is due in part to the muscle wall becoming weaker as we get older and also a small gap in the muscle wall in males where the colon can protrude under stress, making males much more likely to encounter hernias than the female population. Hernias are also more common if you do heavy lifting or are a professional sportsman or woman where the body is under a high degree of physical stress. Neither a physically active nor sedentary lifestyle are contributing factors in themselves.
Types
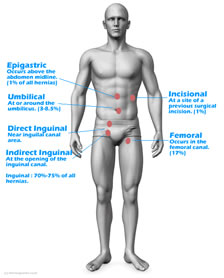
Direct Inguinal
The direct and indirect Inguinal hernias are the most common hernias affecting around 70-75% of all hernia patients affecting far more male patients who are predisposed to this type. A direct inguinal hernia pushes protrudes through the inguinal ring and typically the long-term failure of the inguinal ring to seal after the testicle passes through it. More common in older men.
Indirect Inguinal
An indirect Inguinal hernia protrudes through a weak point in the fascia of the abdominal wall in approximately the same region.
It can occur at any age.
Epigastric
Epigastric hernias are relatively rare with just 1% of the hernia population. Generally classed as above the abdominal midline.
Umbilical
At birth the umbilical cord leaves a weakness in the abdominal wall as the umbilical cord desiccates and disappears. A hernia can then protrude through this weakness. Affects up to 8% of all hernias. The hernia can be retained with a specialist hernia belt.
Incisional
An incisional hernia develops at the site of previous surgery where the muscle wall is already weaker or was previously cut. Friedrich et al recommend weight loss (where necessary) as the principal solution. Incisional hernias are seen in just 1% of all hernia cases.
Femoral
Femoral hernias follow the femoral canal and account for 10% of all hernias. However, due to the smaller space through which the intestine protrudes they present a bigger risk to patient health as the colon has more chance of becoming strangulated and infected. 40% of femoral hernias present as emergencies. Unusually the incidence of femoral hernias is 4 times higher in women than men because a femoral hernia can be caused by pregnancy and childbirth.
Classification of Hernias
Hernias fall into three broad classifications:
-
Reducible - The hernia can be compressed back into the body without undue strain or pain.
-
Incarcerated - cannot be pushed back into the body without strain or pain.
-
Strangulated - The blood supply of the intestinal sac is cut off - normally a medical emergency at this stage (Just 0.2% of cases [2]
Solutions
Surgery - Will typically be recommended where the hernia is having a direct impact on a persons lifestyle. There are two choices which will depend on your surgeons preference and skill set:
-
Endoscopic (keyhole) surgery - generally better outcomes although more expensive. Does not use a mesh.
-
Open mesh repair surgery - more common, cheaper and straightforward but a growing selection of medical evidence that the post operative pain may have been underestimated.
Watchful Waiting - For asymptomatic or minimally symptomatic hernia your doctor may recommend a period of 'watchful waiting'. During this period controlling the hernia together with diet additions can still have good outcomes. In several recent medical trials patient outcomes in terms of quality of life and pain thresholds were similar to patients that had surgery.
Regime Change - In either case, your medical practitioner will probably advise a dietary and health-related regime change so that the hernia is not exacerbated.
Post Surgery
Around 30% of people with a unilateral hernia go on to develop a hernia on the other side so be careful! We recommend that our briefs are worn post-operation when the local area is completely healed and under the direction of your surgeon. (You do not need the foam pad insert).
Inguinal Hernias are an old story.
One of the earliest known descriptions of a hernia comes from the ancient Egyptian medical text called the Edwin Smith Papyrus, which dates back to around 1600 BCE. The papyrus describes a patient with a protrusion in the groin area that is caused by a rupture in the abdominal wall. While the specific type of hernia is not identified, the description is consistent with an inguinal hernia.
In ancient Greece, the physician Hippocrates (c. 460 BCE – c. 370 BCE) described hernias as "ruptures" and suggested that they could be treated by applying pressure to the affected area. Later Greek physicians, such as Galen (129-216 CE), also wrote about hernias and suggested various treatments, including the use of bandages and trusses to support the abdominal wall. There is limited information available about the medical history of historical figures, and it is not always clear whether they suffered from inguinal hernias. However, there are some reports and speculations about famous people who may have had an inguinal hernia.
These include:
Julius Caesar: According to some historians, Julius Caesar may have suffered from an inguinal hernia. He was said to have worn a special belt to support his abdominal muscles during military campaigns. Roman historian Suetonius writes in the 2nd Century...
"He used to wear a belt under his tunic, and constantly girded himself with it in order to support his rather weak constitution and the strain of his campaigns, especially on account of his tendency to abdominal trouble, which was due to a condition of his body that was relaxed and easily upset."
Isaac Newton: It is rumored that Isaac Newton may have had an inguinal hernia, which could have contributed to his reclusive and solitary nature later in life.
Napoleon Bonaparte: Some historians speculate that Napoleon Bonaparte may have had an inguinal hernia, which would explain his
frequent complaints of abdominal pain and his preference for sitting rather than standing.
Harry Houdini: The famous magician and escape artist Harry Houdini is known to have suffered from an inguinal hernia, which he
aggravated during one of his performances.