| Transcript of Inside Health Radio4This BBC Inside Health Transcript describes the rationing of hernia surgery on the UK NHS and some of the short-sighted approaches to save money. If you are struggling to get hernia surgery I am sure you will find it interesting... THE ATTACHED TRANSCRIPT WAS TYPED FROM A RECORDING AND NOT COPIED FROM AN ORIGINAL SCRIPT. BECAUSE OF THE RISK OF MISHEARING AND THE DIFFICULTY IN SOME CASES OF IDENTIFYING INDIVIDUAL SPEAKERS, THE BBC CANNOT VOUCH FOR ITS COMPLETE ACCURACY. INSIDE HEALTH Programme 5. TX: 31.01.17 2100-2130 PRESENTER: MARK PORTER PRODUCER: ERIKA WRIGHT Porter Coming up today carpal tunnel syndrome, hernias and varicose veins and why you might now struggle to get any of them treated on the NHS. And the difficulty is not limited to these common complaints. Clinical Commissioning Groups in the Midlands have been in the headlines this week after raising the bar for eligibility for hip and knee replacements. If you live in Worcestershire your arthritis now needs to be severe enough to cause pain that interferes with daily life and keeps you awake at night. If it’s not then the local CCGs won’t pay for the surgery. A move they believe will lead to 350 fewer operations, saving them around £20 million a year to spend on other therapies they deem higher priority. Prioritisation is otherwise known as rationing and there’s a burgeoning number of interventions on the not normally funded list, produced by CCGs to show what they are not prepared to pay for unless there are exceptional circumstances. Clinicians with patients they regard as special cases with things like hernias have to seek approval using an individual funding request – or IFR – which is appraised by a panel to check the patient meets the necessary criteria. Jonothan Earnshaw is Consultant Surgeon at Cheltenham General Hospital. Earnshaw Groin hernias are very common and the danger with having a groin hernia is strangulation where a piece of bowel gets into the hernia and twists and in that circumstance people need an urgent hernia repair and sometimes even the bowel needs to be removed. And the reason for doing routine elective hernia repair is to prevent strangulation. The problem is it’s really very tricky to assess whether an individual hernia is likely to strangulate and for that reason we’ve ended up in the past operating on most people who have hernias, unless there was a strong reason not to – if someone was very elderly or unfit and very occasionally I suppose we wouldn’t treat minor, small hernias – but essentially all people with hernias had surgery for them. Porter So fast forward to today, what’s the situation now? Earnshaw Well over the last 10 years we’ve certainly had various different protocols that have been given to us to try and reduce the number of hernias that we operate on. Sometimes we’ve been asked to mend just painful ones or sometimes we’ve been asked mend only ones that are likely to strangulate but that’s a very non-specific way of being able to tell the difference between hernias and that’s not very helpful for me to decide whether or not to fix them. Porter And the driver behind that has been what – the clinical evidence base that shows that some hernias don’t need treating, won’t cause trouble or is it mainly a cost issue? Earnshaw The main driver, as with so many of these things, is cost, to reduce the number of hernias that are done that really are never going to strangulate. The science shows actually that if you take people with small hernias and there have been a couple of randomised trials where people either operate on a hernia or select patients for watchful waiting and see what happens over a number of years and if you do that over about 10 years most of the watchful waiting group get bigger and need surgery. Porter So you might be delaying the inevitable with a lot of these patients? Earnshaw I think that’s exactly what you’re doing. Porter But what’s practically involved as a consultant? So I see somebody with a common type of hernia, I send them to you, you then look at them and say I think this needs an operation – what happens? Earnshaw So at the moment the rules have changed. A couple of years ago we all had to fill a form in which was sent to the interventions not normally funded group and they checked the forms to see whether they matched criteria for surgery. Porter So this was even though you decided that the patient needed surgery, somebody else is checking that…? Earnshaw Was checking it, yes, and turning some of them down, saying that they weren’t suitable for repair, particularly those who had direct more mild hernias, if my clinic letter didn’t say that they had severe pain then they were often turned down. Porter So severe pain being one of the boxes you had to tick. Earnshaw Being one of the boxes, absolutely and in a working age person having a hernia, particularly if you’ve got a manual job, can be very uncomfortable. Porter So are you spending a lot of your time now filling in these funding referrals for hernias? Earnshaw No that seems to have stopped and I’ve assumed that the Clinical Commissioning Groups have found that it actually doesn’t reduce the number of people who get operations and therefore that the costs of this layer of bureaucracy actually aren’t worth it. Porter So essentially it might have been that it was an administrative hurdle that wasn’t actually making a lot of difference. Earnshaw Exactly right. Porter How does your practice here compare to practices elsewhere in the country? Are you operating on a similar proportion of the hernias that you see? Earnshaw No, my colleagues around the country tell me that there’s a very big discrepancy between who gets hernia repairs. In some places, like Gloucestershire, it’s pretty easy to get your hernia repaired if there is an appropriate reason for doing so. Porter So that’s your decision. Earnshaw So that’s my decision. What happens for that is that because people are able to travel is they often come over here to get their hernia repaired from neighbouring counties. In many parts of the country it’s extraordinarily difficult to get your hernia repaired and the difficulty of course is to assess which hernias are the ones which are most likely to strangulate, it’s a very difficult clinical decision. Porter But it must be that your colleagues in other parts of the country are wanting to operate on the ones that they think might strangulate, so are they better or worse at selecting them than you or is it an inexact science? Earnshaw It’s a very inexact science and I think it must be deeply frustrating to find that you can only operate on a very small proportion of people with hernias because hernias are uncomfortable and it’s one of the operations I do that people seem to derive most benefit from in terms of improving their symptoms. Porter And if you’re not operating on many people you will, be default, miss some that go on to strangulate. Earnshaw Yes and I would imagine that in areas where you don’t do a lot of elective hernia repairs you will start to see people with strangulated hernias. And fixing a strangulate hernia in an emergency is not an easy thing to do. Porter Surgeon Jonothan Earnshaw. Inside Health’s Margaret McCartney has been looking at what research says about the impact of limiting access to treatments like hernia surgery. McCartney Mark, I have found the evidence, it’s taken me the best part of a week, but I can back this up. In 2009 the Department of Health had asked the management consultancy McKinsey to find out how to make services more cost effective in England and one of the things they proposed was that groin hernias in the main didn’t have to be operated on because mainly people got on just as well if they didn’t have an operation than if they did. And this was proposed as a cost saving device and as a result many CCGs decided to no longer operate routinely for people who had groin hernias that didn’t seem to be causing them much problem. And that might seem on one level absolutely fine, why interfere with something that wasn’t causing you problems anyway? But at that time no one had investigated what the consequences of this new policy would be. Well a group of surgeons went and looked to see what happened in the 16 months before and after this new policy. And what they found was that this policy change made more people who had a hernia, that hadn’t been operated on, end up turning up as an emergency, needing an emergency procedure done on that hernia that had then developed a problem. Porter And in terms of numbers what sort of numbers are we talking about? McCartney Overall it’s still small, so this is not to needlessly alarm people who decided on the basis of a discussion with their doctors or healthcare provider not to have surgery. But what these doctors found that was pretty much a doubling of people needing emergency repairs who hadn’t had the operation done, that was 3.6% versus 5.5%. And what was really important was the people in that group who did need emergency care tended to have more adverse effects, more problems after the surgery compared with people who’d had it done routinely. That’s the big problem. Porter Knowing how cynical our Inside Health audience is I suppose my next question should be – well surgeons would say that wouldn’t they? McCartney Mark, I like the cynicism, I support cynicism myself but this was just number counting, this was just looking at what happened afterwards. So I think in this study there was a limited chance of bias. Porter So we’re looking at something like just under one in 20 people needing to have emergency surgery, if – if they were left. McCartney Yeah, now we can’t prove cause and effect, this wasn’t a randomised control trial, it was a study looking at the association of a new policy but it’s the best data we have and that is flagging up a problem. Now it’s completely different if people are sitting down talking about what to do about a problem and making a valid decision based on individual judgement about a set of circumstances. The big problem is that McKinsey, who made the recommendation not to routinely operate on people with inguinal hernias, they based this policy on trials that were done from America, but the trials are flawed when we start to compare with them with practice in the UK of enforcing this policy because over half the people offered entry into the trials didn’t take part in it, they declined to do so, they wanted to have surgery anyway. So we cannot compare like with like, we cannot say that therefore this policy is going to benefit our patients in the UK, the data was flawed. Porter So the findings of the research might have been skewed by the people who were included in the trial but you’re confident that this second trial, where the surgeons went to look to see what happened to these people, that that was reflective of real life practice? McCartney Well this is real life practice, it’s not a clinical trial, we can’t prove cause and effect but we certainly can say that this policy was associated with a change in the amount of people who presented as an emergency. Porter Margaret McCartney. Hand surgery is another area that has been targeted by CCGs looking to save resources. Ash Merry’s specialist had to apply for funding when he felt she needed surgery for carpal tunnel syndrome – a common complaint caused by entrapment of one of the nerves supplying the hand. And it was giving her a lot of trouble. Merry Pins and needles. Not during the day but specifically at night. And I used to lie in bed, put my hands above my head and I was kept awake literally by the pain in my right hand and it is excruciating, it’s like electric shocks going up and down your arm and you cannot stop it. It was quite literally wrecking my life I felt. Porter And how long had that been going on before you first sought medical advice? Merry Not sleeping at night, it has been going on intermittently probably for about a year. Porter So you went to see your doctor? Merry Yes. I went to see the doctor in March 2016 and I went to see a consultant before Christmas and I thought ooh this is to check yes what surgery’s going to be. No it wasn’t. We have to now apply for funding. Porter Had you ever heard of anything like this happening before? Merry No, I jolly well hadn’t. Pailthorpe So I’m Charles Pailthorpe, I’m a Consultant Orthopaedic Surgeon with a specialist interest in the hand at the Royal Berkshire Hospital in Reading. My practice as a hand surgeon has changed quite dramatically over the past couple of years with the individual funding requests policy. It’s become almost an administrative nightmare, having to spend more and more time filling in forms, I don’t think it’s got any benefit to my patients at all. And the problem in hand surgery is that it affects almost half my practice, so simple, in relative terms, conditions called carpal tunnel syndrome, which is a trapped nerve, things like a trigger finger where the finger gets caught and a condition called Dupuytren’s where the finger actually gets stuck – these are common hand conditions but now have to have funding requested. CCGs have stated in their funding request information that exceptional health requirement is over and above what is there for the general public. But if you’ve got a condition that’s affecting your life and stopping you either from sleeping, like carpal tunnel syndrome or you’re unable to do your job because you can’t feel your hands and you’re dropping things why is that exceptional above the general public? It’s not and so this rationing purposes doesn’t take into effect what’s happening to the actual patient themselves. And so from my perspective my job is to treat the patient and each patient who uses their hands is individual, we’re all individuals, we all use our hands, we all abuse our hands but we all do it differently. So what is a problem for one person isn’t for somebody else. And so actually having a checklist of so-called interventions before you can do surgery doesn’t make sense for an individual where there may well be exceptional reasons. So I’m having my professional integrity in essence questioned by having to prove exceptional health requirements. Porter Is that part of it though, I mean that you feel that you’re being undermined professionally, I mean is that one of the reasons that I mean it gets your goat, I can feel it? Pailthorpe You know I’ve been a hand surgeon since 1995, I think I’m not a knife happy surgeon, I’m a very cautious surgeon but when I do make a decision with the patient’s agreement that surgery’s appropriate I’d like to feel that I have the professional integrity that that’s correct. Porter Looking at carpal tunnel syndrome, it’s a common problem, we see a lot of it in general practice, refer a lot of it to surgeons like you, how many of the patients that you feel definitely need an operation do you get approved easily or are you constantly getting refusals? Pailthorpe We think that we’re probably getting about a 20% rejection rate and that’s largely based on a failure of the checklist concept. So if they haven’t had a splint or if they haven’t had an injection it’s often rejected, they say why haven’t they had an injection, despite the fact that I’ve put down sometimes the reason why I think an injection’s not appropriate, because there are sometimes reasons, they’ve still be rejected. Porter Because that’s the other part of the rationalisation isn’t it, it’s not just about saving resources but it’s using resources appropriately and getting people to follow guidelines. So for instance with carpal tunnel they might get somebody like me to say we’ll try a splint for four to six weeks first, then refer to you, you might consider an injection and then surgery as a last resort. Pailthorpe Well I don’t have a problem with that actually but there are exceptions. What we haven’t got at the moment is a way of agreeing those exceptions with the clinical groups. For example, in carpal tunnel syndrome if somebody’s got wasting of their thumb muscles that should be just let through, we shouldn’t have to apply for funding. Porter They need an operation. Pailthorpe Yeah, they need an operation, it’s a barn door decision, you just need to get on and get it done sort of thing. Merry I have paid contributions for 37 years, I can understand that good housekeeping is vital, however, when it comes to something like carpal tunnel surgery, as I understand it, when it is severe whatever you do to it at some stage surgery is going to be needed. To stop the progression of impairment in your dominant hand I would argue that any delay could be more costly to the NHS. Porter So what happened in your case? Merry Well what happened in my case is I have to say I made a bit of a noise. I was constantly chasing it. So when funding was approved the process was really remarkably quick. I’ve since found out there are vacant surgery slots that are not being filled with staff on standby, which is costing money, that are going vacant because they were waiting for funding requests to be approved. Pailthorpe To me it’s almost as if some days they’ve used their quota up because it seems to be completely irrational – other ones go through without a problem and then I’ll get one rejected. Porter What happens to those 20% of patients, what’s the risk of not operating on somebody like Ash? Pailthorpe Well the risk in her case in fact is that the pressure on the nerve cause permanent damage. Porter So looking at those 20% that are refused are any of them ever going to get better on their own or are they going to end up under your care having an operation at some stage? Pailthorpe I don’t think it ever goes. The trouble is that the literature is confusing sometimes when it comes to certain treatments, particularly when it comes to simple things like carpal tunnel because sometimes there isn’t an awful lot of evidence but there’s an awful lot of common sense and experience. Porter Because this is one of the areas that the people behind these criteria will say look there isn’t enough evidence to support this intervention and what you’re saying is it’s just because there isn’t enough evidence. It might be that the trials haven’t been done, it’s not that the procedure doesn’t work – is that what you’re saying? Pailthorpe Yeah to a certain extent yes. Though there is, I think, more evidence coming out. There is a big study in fact in Sweden on corticosteroid injections and showed that again in certain specific instances is actually a very effective treatment and will reduce the symptoms for a year or more, though… Porter But is it delaying the inevitable? Pailthorpe They eventually all still come to surgery at some point because nobody has followed them up for another 10 years. And so that’s why the evidence is fundamentally flawed and I do have some patients who grumble along for years, have had some ladies who’ve come to me in their 50s, 60s and said well I’ve had it for 20 years but now actually I can’t feel my fingers. Well it’s almost too late then. So there comes a time where actually there is an opportune time to get on with it. Porter What’s happening in other parts of the country, is this something that’s happening pretty uniformly? Pailthorpe No I don’t think so, it seems to me that there are – some of my colleagues I’ve chatted to they say well what are IFRs – individual funding requests – they don’t have to do them. So some parts of the country it’s not active at the moment but other parts it’s obviously almost draconian. Porter Ash mentioned empty slots where because the funding’s not coming through there’s a slot that could have been used but the team’s all still there, is that actually happening? Pailthorpe Yes. We were planning to do a list at the end of January and we have something I think in the region of 40-50 patients where we’re waiting on funding. So it was all set to go but we just haven’t got the patients at the moment to fill the list. Overall there’s a lot of waste of money in this process. We’ve had to employ an administrative staff just for IFRs! Porter Charles Pailthorpe and his patient Ash Merry. Back in Cheltenham surgeon Jonothan Earnshaw treats varicose veins as well as hernias, and he too has witnessed a dramatic change in practice over recent years. His team now does half the operations it used to. Earnshaw Over the years there’s been an increasing thought that in fact a lot of varicose veins don’t need to be done – they’re either cosmetic or there’s no medical advantage in doing them – and so we’ve had great restrictions on the sort of veins that we can treat. So we tend now only to be allowed to treat people who’ve got complications from their veins, not just simple discomfort. Porter And the sort of complications that you’d have to have – the boxes that you’d have to tick – to get approved for your surgery would be what? Earnshaw So if you have varicose veins long enough they start to affect the skin around your ankle and you’ve seen the brown speckling there which is called varicose eczema and that’s a sign that there’s high pressure in the veins of the skin. If you don’t treat people with varicose eczema there’s a high chance if they damage their skin they will get a varicose ulcer and varicose ulcers are common particularly in the elderly. So the idea of treating people with varicose veins is to prevent them getting the complications of varicose ulcer. Porter And presumably once somebody develops that complication that’s expensive and difficult to deal with? Earnshaw Oh yes and painful, it’s horrible having a varicose ulcer, it really grossly affects quality of life. And most of the guidelines and restrictions on treatment for varicose veins allow treatment of people with complicated varicose veins for that very reason. And the guidelines for varicose veins are much easier because the classification of varicose veins is easier. It’s obvious when people are starting to get complications in their veins – and those are the ones we treat – it’s obvious which are the ones don’t have complications and those generally speaking are the ones that we don’t treat. Porter Are you happy with where the bar is set? Earnshaw Well again the bar is very variable around the country. Here in Gloucestershire we’re allowed to treat people with complicated varicose veins and people whose varicose veins severely affect their quality of life. The problem of course is who decides whether a quality of life is severely affected and we often end up having quite uncomfortable consultations in outpatients where perhaps my perception of quality of life isn’t quite the same as the person who has their varicose veins and that can lead to considerable difficulty. Porter So will you sometimes tell a patient in outpatients look you’re not going to meet the threshold, we’re not going to be able to operate on you or we don’t need to operate on you? Earnshaw That happens in every clinic that I do. We have people who come with what they regard as severe symptoms from their varicose veins but actually when you question them they’re not affecting their sleep, they don’t require painkillers, they’re not actually affecting their work and under those circumstances our local commissioning wouldn’t fund that intervention. So I have to tell patients then that I can’t operate on their veins. Porter But what happens to them if you don’t operate on their veins, I mean they’re not going to get better are they, I mean presumably with time they get worse – do they – are we just delaying the inevitable here as well? Earnshaw Well that’s not quite the case because as a GP you’ll have had many patients who have varicose veins for years and years and years and years and years that never ever get any complications and if we could predict which people with varicose veins were going to go on and get complications then it would be easy to select those out but we can’t and most people don’t get complications from their varicose veins. So there are reasonable medicine reasons for not operating, not treating people with varicose veins, until they actually start to get the complications.
Porter So what might happen is a patient might be referred into you, you say don’t need to operate, or can’t operate now, come back when you’ve got a complication for those that do? Earnshaw Exactly right and as a surgeon who’s been in one place for a very long time that happens not infrequently. But of course the corollary of that is that I’ve sent away a lot of people and reassured them their veins are no threat to their health and they’ve never come back over the years. Porter Jonothan Earnshaw. Clinical Commissioning Groups - CCGs - are in a difficult position, squeezed between the expectations of their public and the demands of their doctors and other healthcare professionals. Buckinghamshire GP Graham Jackson is Chair of his local CCG, and co-Chair of NHS Clinical Commissioners. Jackson Clinical Commissioning Groups are allocated a certain amount of resource from central government to spend on healthcare in their locality or their area. And what we have to do is decide how to spend that resource most effectively. Cancer services, emergency services, surgical interventions – and so we have to make decisions based on the population and remembering the populations differ from different parts of the country and then how we spend that money is based on their local need. Porter And put simply, if you spend more money on people having minor varicose veins treated, for instance, that leaves you less money to help people who might have severe arthritis and require a hip replacement? Jackson Well it’s certainly true there’s only a finite fixed amount of fund. Porter One of the criticisms aimed at the current set up is that there’s something of what’s become known as the postcode lottery, that if the criteria for all of these procedures, for getting your hand surgery done, your varicose veins done or your hip done was the same in every area of the country and people understand there are limited resources then perhaps everyone would buy into it much more. Why is there this variability? Jackson I think the variability comes back to the fact that we are locally focused and so the priorities for spending healthcare in a particular area need to be matched to the priority of that population and it’s really important to understand that the local population has different needs from different parts of the country, even actually in say the same county in different areas based on their age profile etc. Porter And are some CCGs under more financial pressures than others because of that change in demography? Jackson I think that is true. There is an allocation across the country from CCG to CCG based on that profile but it’s very difficult to make those allocations absolutely accurate everywhere. Porter One of the concerns, I suppose, is that we are delaying the inevitable, so that by reducing perhaps the number of hernias that we operate on we end up maybe with more people coming in with strangulations that are expensive and obviously have implications for the patient. I presume we’re monitoring this situation ongoing to check that these interventions are cost effective in the long term? Jackson Yes there’s a lot of monitoring going on in the number of interventions but I think it comes back to the whole picture again – we have an ageing population with an increasing number of illnesses that need to be dealt with. Porter Do you know for sure that your gateways, if you like, to limit the treatments that are being done, to prioritise the treatments that are being done, actually work in terms of cost effectiveness, that they’re saving your CCG money? Jackson I think there is monitoring within the system and clearly there’s a cost for those gateways and we have to be honest there is a cost to run those gateways and it’s important that those costs are monitored against the cost of procedures. Porter Because it might be that a particular gateway that’s put in with all the best intentions might end up not working, it might not be cost effective to do that but to make that decision you need to be monitoring these very closely and that is going on is it across the country? Jackson It is going on and then there is clearly – everything we do has a cost attached to it and the basic premise is that we have limited resource and we must not squander that resource.
Porter Yes I mean we mustn’t squander it on unnecessary treatments but we mustn’t squander it on unnecessary admin but we’re looking at the treatments from an evidence base – I mean I’m just asking are we applying those same stringent rules to the gateway interventions, to the admin behind this?
Jackson The gateway interventions are monitored monetarily but also from a quality perspective to make sure they do provide the quality assessment that we need.
Porter Dr Graham Jackson. So given that CCGs across England are monitoring the impact of prioritising treatments like hernia repairs, and hand and varicose vein surgery, we went looking for published examples of their findings. When I say we….
McCartney Mark, I may never forgive you for this. I’ve spent the last week trawling through minutes from CCGs looking to see who is looking at the harms of the procedures that people have put in place to try and limit access to interventions. I can find almost none. I can find people that have written down things like – Will this affect people, for example, older people more or carers more, qualities analysis, but I cannot find any analysis done of the cost effectiveness of the entire procedure.
Porter Well Graham says it’s being monitored, so one would imagine that if his CCG’s doing that that that’s happening across the country but what you’re saying is that nothing is being published?
McCartney I can’t find anything in the public domain, if any listeners know of any please do send it in for me. And of course there’s all sorts of other costs associated with not doing things, for example people having more physiotherapy, people attending their GP more to get painkillers, people being off work, people maybe needing to see a psychologist, people not being able to care for family or relatives. These costs, I think, are being absorbed elsewhere into the system and they’re not being properly tabulated.
Porter And of course the other aspect is the cost of the bureaucracy itself, which needs to be balanced against the cost of not doing some of these operations.
McCartney Yeah, ask GPs how much time they’re spending doing paperwork as opposed to face to face patient care – it’s huge and it’s growing and I don’t think anyone’s really got a clear handle on how much of this is being generated by CCGs and these type of rules.
Porter But we can’t be dismissive of it because we don’t know because the evidence isn’t published?
McCartney And that’s a big problem, whenever you’re putting a new policy into practice I think it should be incumbent on the policymakers to say what are the potential harms, what are the potential downsides and how are we going to find out about them because if you don’t look for them you will not find them, they will be buried and they’ll just come back to bite you on the posterior later on.
Porter Margaret McCartney – who will be one of the panellists in our upcoming hour long special debate on the NHS – what needs to give? – which will be aired on Valentine’s day. In the meantime normal service resumes next week when I will learning how virtual reality is being used to help people with conditions as diverse as Alzheimer’s disease and phantom limb pain. As well as taking a closer look at the latest initiative to limit and target antibiotic use for sore throats.
ENDSTHE ATTACHED TRANSCRIPT WAS TYPED FROM A RECORDING AND NOT COPIED FROM AN ORIGINAL SCRIPT. BECAUSE OF THE RISK OF MISHEARING AND THE DIFFICULTY IN SOME CASES OF IDENTIFYING INDIVIDUAL SPEAKERS, THE BBC CANNOT VOUCH FOR ITS COMPLETE ACCURACY.
INSIDE HEALTH
Programme 5.
TX: 31.01.17 2100-2130
PRESENTER: MARK PORTER
PRODUCER: ERIKA WRIGHT
Porter Coming up today carpal tunnel syndrome, hernias and varicose veins and why you might now struggle to get any of them treated on the NHS.
And the difficulty is not limited to these common complaints. Clinical Commissioning Groups in the Midlands have been in the headlines this week after raising the bar for eligibility for hip and knee replacements. If you live in Worcestershire your arthritis now needs to be severe enough to cause pain that interferes with daily life and keeps you awake at night. If it’s not then the local CCGs won’t pay for the surgery. A move they believe will lead to 350 fewer operations, saving them around £20 million a year to spend on other therapies they deem higher priority.
Prioritisation is otherwise known as rationing and there’s a burgeoning number of interventions on the not normally funded list, produced by CCGs to show what they are not prepared to pay for unless there are exceptional circumstances.
Clinicians with patients they regard as special cases with things like hernias have to seek approval using an individual funding request – or IFR – which is appraised by a panel to check the patient meets the necessary criteria.
Jonothan Earnshaw is Consultant Surgeon at Cheltenham General Hospital.
Earnshaw Groin hernias are very common and the danger with having a groin hernia is strangulation where a piece of bowel gets into the hernia and twists and in that circumstance people need an urgent hernia repair and sometimes even the bowel needs to be removed. And the reason for doing routine elective hernia repair is to prevent strangulation. The problem is it’s really very tricky to assess whether an individual hernia is likely to strangulate and for that reason we’ve ended up in the past operating on most people who have hernias, unless there was a strong reason not to – if someone was very elderly or unfit and very occasionally I suppose we wouldn’t treat minor, small hernias – but essentially all people with hernias had surgery for them.
Porter So fast forward to today, what’s the situation now?
Earnshaw Well over the last 10 years we’ve certainly had various different protocols that have been given to us to try and reduce the number of hernias that we operate on. Sometimes we’ve been asked to mend just painful ones or sometimes we’ve been asked mend only ones that are likely to strangulate but that’s a very non-specific way of being able to tell the difference between hernias and that’s not very helpful for me to decide whether or not to fix them.
Porter And the driver behind that has been what – the clinical evidence base that shows that some hernias don’t need treating, won’t cause trouble or is it mainly a cost issue?
Earnshaw The main driver, as with so many of these things, is cost, to reduce the number of hernias that are done that really are never going to strangulate. The science shows actually that if you take people with small hernias and there have been a couple of randomised trials where people either operate on a hernia or select patients for watchful waiting and see what happens over a number of years and if you do that over about 10 years most of the watchful waiting group get bigger and need surgery.
Porter So you might be delaying the inevitable with a lot of these patients?
Earnshaw I think that’s exactly what you’re doing.
Porter But what’s practically involved as a consultant? So I see somebody with a common type of hernia, I send them to you, you then look at them and say I think this needs an operation – what happens?
Earnshaw So at the moment the rules have changed. A couple of years ago we all had to fill a form in which was sent to the interventions not normally funded group and they checked the forms to see whether they matched criteria for surgery.
Porter So this was even though you decided that the patient needed surgery, somebody else is checking that…?
Earnshaw Was checking it, yes, and turning some of them down, saying that they weren’t suitable for repair, particularly those who had direct more mild hernias, if my clinic letter didn’t say that they had severe pain then they were often turned down.
Porter So severe pain being one of the boxes you had to tick.
Earnshaw Being one of the boxes, absolutely and in a working age person having a hernia, particularly if you’ve got a manual job, can be very uncomfortable.
Porter So are you spending a lot of your time now filling in these funding referrals for hernias?
Earnshaw No that seems to have stopped and I’ve assumed that the Clinical Commissioning Groups have found that it actually doesn’t reduce the number of people who get operations and therefore that the costs of this layer of bureaucracy actually aren’t worth it.
Porter So essentially it might have been that it was an administrative hurdle that wasn’t actually making a lot of difference.
Earnshaw Exactly right.
Porter How does your practice here compare to practices elsewhere in the country? Are you operating on a similar proportion of the hernias that you see?
Earnshaw No, my colleagues around the country tell me that there’s a very big discrepancy between who gets hernia repairs. In some places, like Gloucestershire, it’s pretty easy to get your hernia repaired if there is an appropriate reason for doing so.
Porter So that’s your decision.
Earnshaw So that’s my decision. What happens for that is that because people are able to travel is they often come over here to get their hernia repaired from neighbouring counties. In many parts of the country it’s extraordinarily difficult to get your hernia repaired and the difficulty of course is to assess which hernias are the ones which are most likely to strangulate, it’s a very difficult clinical decision.
Porter But it must be that your colleagues in other parts of the country are wanting to operate on the ones that they think might strangulate, so are they better or worse at selecting them than you or is it an inexact science?
Earnshaw It’s a very inexact science and I think it must be deeply frustrating to find that you can only operate on a very small proportion of people with hernias because hernias are uncomfortable and it’s one of the operations I do that people seem to derive most benefit from in terms of improving their symptoms.
Porter And if you’re not operating on many people you will, be default, miss some that go on to strangulate.
Earnshaw Yes and I would imagine that in areas where you don’t do a lot of elective hernia repairs you will start to see people with strangulated hernias. And fixing a strangulate hernia in an emergency is not an easy thing to do.
Porter Surgeon Jonothan Earnshaw.
Inside Health’s Margaret McCartney has been looking at what research says about the impact of limiting access to treatments like hernia surgery.
McCartney Mark, I have found the evidence, it’s taken me the best part of a week, but I can back this up. In 2009 the Department of Health had asked the management consultancy McKinsey to find out how to make services more cost effective in England and one of the things they proposed was that groin hernias in the main didn’t have to be operated on because mainly people got on just as well if they didn’t have an operation than if they did. And this was proposed as a cost saving device and as a result many CCGs decided to no longer operate routinely for people who had groin hernias that didn’t seem to be causing them much problem. And that might seem on one level absolutely fine, why interfere with something that wasn’t causing you problems anyway? But at that time no one had investigated what the consequences of this new policy would be. Well a group of surgeons went and looked to see what happened in the 16 months before and after this new policy. And what they found was that this policy change made more people who had a hernia, that hadn’t been operated on, end up turning up as an emergency, needing an emergency procedure done on that hernia that had then developed a problem.
Porter And in terms of numbers what sort of numbers are we talking about?
McCartney Overall it’s still small, so this is not to needlessly alarm people who decided on the basis of a discussion with their doctors or healthcare provider not to have surgery. But what these doctors found that was pretty much a doubling of people needing emergency repairs who hadn’t had the operation done, that was 3.6% versus 5.5%. And what was really important was the people in that group who did need emergency care tended to have more adverse effects, more problems after the surgery compared with people who’d had it done routinely. That’s the big problem.
Porter Knowing how cynical our Inside Health audience is I suppose my next question should be – well surgeons would say that wouldn’t they?
McCartney Mark, I like the cynicism, I support cynicism myself but this was just number counting, this was just looking at what happened afterwards. So I think in this study there was a limited chance of bias.
Porter So we’re looking at something like just under one in 20 people needing to have emergency surgery, if – if they were left.
McCartney Yeah, now we can’t prove cause and effect, this wasn’t a randomised control trial, it was a study looking at the association of a new policy but it’s the best data we have and that is flagging up a problem. Now it’s completely different if people are sitting down talking about what to do about a problem and making a valid decision based on individual judgement about a set of circumstances. The big problem is that McKinsey, who made the recommendation not to routinely operate on people with inguinal hernias, they based this policy on trials that were done from America, but the trials are flawed when we start to compare with them with practice in the UK of enforcing this policy because over half the people offered entry into the trials didn’t take part in it, they declined to do so, they wanted to have surgery anyway. So we cannot compare like with like, we cannot say that therefore this policy is going to benefit our patients in the UK, the data was flawed.
Porter So the findings of the research might have been skewed by the people who were included in the trial but you’re confident that this second trial, where the surgeons went to look to see what happened to these people, that that was reflective of real life practice?
McCartney Well this is real life practice, it’s not a clinical trial, we can’t prove cause and effect but we certainly can say that this policy was associated with a change in the amount of people who presented as an emergency.
Porter Margaret McCartney.
Hand surgery is another area that has been targeted by CCGs looking to save resources. Ash Merry’s specialist had to apply for funding when he felt she needed surgery for carpal tunnel syndrome – a common complaint caused by entrapment of one of the nerves supplying the hand. And it was giving her a lot of trouble.
Merry Pins and needles. Not during the day but specifically at night. And I used to lie in bed, put my hands above my head and I was kept awake literally by the pain in my right hand and it is excruciating, it’s like electric shocks going up and down your arm and you cannot stop it. It was quite literally wrecking my life I felt.
Porter And how long had that been going on before you first sought medical advice?
Merry Not sleeping at night, it has been going on intermittently probably for about a year.
Porter So you went to see your doctor?
Merry Yes. I went to see the doctor in March 2016 and I went to see a consultant before Christmas and I thought ooh this is to check yes what surgery’s going to be. No it wasn’t. We have to now apply for funding.
Porter Had you ever heard of anything like this happening before?
Merry No, I jolly well hadn’t.
Pailthorpe So I’m Charles Pailthorpe, I’m a Consultant Orthopaedic Surgeon with a specialist interest in the hand at the Royal Berkshire Hospital in Reading. My practice as a hand surgeon has changed quite dramatically over the past couple of years with the individual funding requests policy. It’s become almost an administrative nightmare, having to spend more and more time filling in forms, I don’t think it’s got any benefit to my patients at all. And the problem in hand surgery is that it affects almost half my practice, so simple, in relative terms, conditions called carpal tunnel syndrome, which is a trapped nerve, things like a trigger finger where the finger gets caught and a condition called Dupuytren’s where the finger actually gets stuck – these are common hand conditions but now have to have funding requested. CCGs have stated in their funding request information that exceptional health requirement is over and above what is there for the general public. But if you’ve got a condition that’s affecting your life and stopping you either from sleeping, like carpal tunnel syndrome or you’re unable to do your job because you can’t feel your hands and you’re dropping things why is that exceptional above the general public? It’s not and so this rationing purposes doesn’t take into effect what’s happening to the actual patient themselves.
And so from my perspective my job is to treat the patient and each patient who uses their hands is individual, we’re all individuals, we all use our hands, we all abuse our hands but we all do it differently. So what is a problem for one person isn’t for somebody else. And so actually having a checklist of so-called interventions before you can do surgery doesn’t make sense for an individual where there may well be exceptional reasons. So I’m having my professional integrity in essence questioned by having to prove exceptional health requirements.
Porter Is that part of it though, I mean that you feel that you’re being undermined professionally, I mean is that one of the reasons that I mean it gets your goat, I can feel it?
Pailthorpe You know I’ve been a hand surgeon since 1995, I think I’m not a knife happy surgeon, I’m a very cautious surgeon but when I do make a decision with the patient’s agreement that surgery’s appropriate I’d like to feel that I have the professional integrity that that’s correct.
Porter Looking at carpal tunnel syndrome, it’s a common problem, we see a lot of it in general practice, refer a lot of it to surgeons like you, how many of the patients that you feel definitely need an operation do you get approved easily or are you constantly getting refusals?
Pailthorpe We think that we’re probably getting about a 20% rejection rate and that’s largely based on a failure of the checklist concept. So if they haven’t had a splint or if they haven’t had an injection it’s often rejected, they say why haven’t they had an injection, despite the fact that I’ve put down sometimes the reason why I think an injection’s not appropriate, because there are sometimes reasons, they’ve still be rejected.
Porter Because that’s the other part of the rationalisation isn’t it, it’s not just about saving resources but it’s using resources appropriately and getting people to follow guidelines. So for instance with carpal tunnel they might get somebody like me to say we’ll try a splint for four to six weeks first, then refer to you, you might consider an injection and then surgery as a last resort.
Pailthorpe Well I don’t have a problem with that actually but there are exceptions. What we haven’t got at the moment is a way of agreeing those exceptions with the clinical groups. For example, in carpal tunnel syndrome if somebody’s got wasting of their thumb muscles that should be just let through, we shouldn’t have to apply for funding.
Porter They need an operation.
Pailthorpe Yeah, they need an operation, it’s a barn door decision, you just need to get on and get it done sort of thing.
Merry I have paid contributions for 37 years, I can understand that good housekeeping is vital, however, when it comes to something like carpal tunnel surgery, as I understand it, when it is severe whatever you do to it at some stage surgery is going to be needed. To stop the progression of impairment in your dominant hand I would argue that any delay could be more costly to the NHS.
Porter So what happened in your case?
Merry Well what happened in my case is I have to say I made a bit of a noise. I was constantly chasing it. So when funding was approved the process was really remarkably quick. I’ve since found out there are vacant surgery slots that are not being filled with staff on standby, which is costing money, that are going vacant because they were waiting for funding requests to be approved.
Pailthorpe To me it’s almost as if some days they’ve used their quota up because it seems to be completely irrational – other ones go through without a problem and then I’ll get one rejected.
Porter What happens to those 20% of patients, what’s the risk of not operating on somebody like Ash?
Pailthorpe Well the risk in her case in fact is that the pressure on the nerve cause permanent damage.
Porter So looking at those 20% that are refused are any of them ever going to get better on their own or are they going to end up under your care having an operation at some stage?
Pailthorpe I don’t think it ever goes. The trouble is that the literature is confusing sometimes when it comes to certain treatments, particularly when it comes to simple things like carpal tunnel because sometimes there isn’t an awful lot of evidence but there’s an awful lot of common sense and experience.
Porter Because this is one of the areas that the people behind these criteria will say look there isn’t enough evidence to support this intervention and what you’re saying is it’s just because there isn’t enough evidence. It might be that the trials haven’t been done, it’s not that the procedure doesn’t work – is that what you’re saying?
Pailthorpe Yeah to a certain extent yes. Though there is, I think, more evidence coming out. There is a big study in fact in Sweden on corticosteroid injections and showed that again in certain specific instances is actually a very effective treatment and will reduce the symptoms for a year or more, though…
Porter But is it delaying the inevitable?
Pailthorpe They eventually all still come to surgery at some point because nobody has followed them up for another 10 years. And so that’s why the evidence is fundamentally flawed and I do have some patients who grumble along for years, have had some ladies who’ve come to me in their 50s, 60s and said well I’ve had it for 20 years but now actually I can’t feel my fingers. Well it’s almost too late then. So there comes a time where actually there is an opportune time to get on with it.
Porter What’s happening in other parts of the country, is this something that’s happening pretty uniformly?
Pailthorpe No I don’t think so, it seems to me that there are – some of my colleagues I’ve chatted to they say well what are IFRs – individual funding requests – they don’t have to do them. So some parts of the country it’s not active at the moment but other parts it’s obviously almost draconian.
Porter Ash mentioned empty slots where because the funding’s not coming through there’s a slot that could have been used but the team’s all still there, is that actually happening?
Pailthorpe Yes. We were planning to do a list at the end of January and we have something I think in the region of 40-50 patients where we’re waiting on funding. So it was all set to go but we just haven’t got the patients at the moment to fill the list. Overall there’s a lot of waste of money in this process. We’ve had to employ an administrative staff just for IFRs!
Porter Charles Pailthorpe and his patient Ash Merry.
Back in Cheltenham surgeon Jonothan Earnshaw treats varicose veins as well as hernias, and he too has witnessed a dramatic change in practice over recent years. His team now does half the operations it used to.
Earnshaw Over the years there’s been an increasing thought that in fact a lot of varicose veins don’t need to be done – they’re either cosmetic or there’s no medical advantage in doing them – and so we’ve had great restrictions on the sort of veins that we can treat. So we tend now only to be allowed to treat people who’ve got complications from their veins, not just simple discomfort.
Porter And the sort of complications that you’d have to have – the boxes that you’d have to tick – to get approved for your surgery would be what?
Earnshaw So if you have varicose veins long enough they start to affect the skin around your ankle and you’ve seen the brown speckling there which is called varicose eczema and that’s a sign that there’s high pressure in the veins of the skin. If you don’t treat people with varicose eczema there’s a high chance if they damage their skin they will get a varicose ulcer and varicose ulcers are common particularly in the elderly. So the idea of treating people with varicose veins is to prevent them getting the complications of varicose ulcer.
Porter And presumably once somebody develops that complication that’s expensive and difficult to deal with?
Earnshaw Oh yes and painful, it’s horrible having a varicose ulcer, it really grossly affects quality of life. And most of the guidelines and restrictions on treatment for varicose veins allow treatment of people with complicated varicose veins for that very reason. And the guidelines for varicose veins are much easier because the classification of varicose veins is easier. It’s obvious when people are starting to get complications in their veins – and those are the ones we treat – it’s obvious which are the ones don’t have complications and those generally speaking are the ones that we don’t treat.
Porter Are you happy with where the bar is set?
Earnshaw Well again the bar is very variable around the country. Here in Gloucestershire we’re allowed to treat people with complicated varicose veins and people whose varicose veins severely affect their quality of life. The problem of course is who decides whether a quality of life is severely affected and we often end up having quite uncomfortable consultations in outpatients where perhaps my perception of quality of life isn’t quite the same as the person who has their varicose veins and that can lead to considerable difficulty.
Porter So will you sometimes tell a patient in outpatients look you’re not going to meet the threshold, we’re not going to be able to operate on you or we don’t need to operate on you?
Earnshaw That happens in every clinic that I do. We have people who come with what they regard as severe symptoms from their varicose veins but actually when you question them they’re not affecting their sleep, they don’t require painkillers, they’re not actually affecting their work and under those circumstances our local commissioning wouldn’t fund that intervention. So I have to tell patients then that I can’t operate on their veins.
Porter But what happens to them if you don’t operate on their veins, I mean they’re not going to get better are they, I mean presumably with time they get worse – do they – are we just delaying the inevitable here as well?
Earnshaw Well that’s not quite the case because as a GP you’ll have had many patients who have varicose veins for years and years and years and years and years that never ever get any complications and if we could predict which people with varicose veins were going to go on and get complications then it would be easy to select those out but we can’t and most people don’t get complications from their varicose veins. So there are reasonable medicine reasons for not operating, not treating people with varicose veins, until they actually start to get the complications.
Porter So what might happen is a patient might be referred into you, you say don’t need to operate, or can’t operate now, come back when you’ve got a complication for those that do?
Earnshaw Exactly right and as a surgeon who’s been in one place for a very long time that happens not infrequently. But of course the corollary of that is that I’ve sent away a lot of people and reassured them their veins are no threat to their health and they’ve never come back over the years.
Porter Jonothan Earnshaw.
Clinical Commissioning Groups - CCGs - are in a difficult position, squeezed between the expectations of their public and the demands of their doctors and other healthcare professionals.
Buckinghamshire GP Graham Jackson is Chair of his local CCG, and co-Chair of NHS Clinical Commissioners.
Jackson Clinical Commissioning Groups are allocated a certain amount of resource from central government to spend on healthcare in their locality or their area. And what we have to do is decide how to spend that resource most effectively. Cancer services, emergency services, surgical interventions – and so we have to make decisions based on the population and remembering the populations differ from different parts of the country and then how we spend that money is based on their local need.
Porter And put simply, if you spend more money on people having minor varicose veins treated, for instance, that leaves you less money to help people who might have severe arthritis and require a hip replacement?
Jackson Well it’s certainly true there’s only a finite fixed amount of fund.
Porter One of the criticisms aimed at the current set up is that there’s something of what’s become known as the postcode lottery, that if the criteria for all of these procedures, for getting your hand surgery done, your varicose veins done or your hip done was the same in every area of the country and people understand there are limited resources then perhaps everyone would buy into it much more. Why is there this variability?
Jackson I think the variability comes back to the fact that we are locally focused and so the priorities for spending healthcare in a particular area need to be matched to the priority of that population and it’s really important to understand that the local population has different needs from different parts of the country, even actually in say the same county in different areas based on their age profile etc.
Porter And are some CCGs under more financial pressures than others because of that change in demography?
Jackson I think that is true. There is an allocation across the country from CCG to CCG based on that profile but it’s very difficult to make those allocations absolutely accurate everywhere.
Porter One of the concerns, I suppose, is that we are delaying the inevitable, so that by reducing perhaps the number of hernias that we operate on we end up maybe with more people coming in with strangulations that are expensive and obviously have implications for the patient. I presume we’re monitoring this situation ongoing to check that these interventions are cost effective in the long term?
Jackson Yes there’s a lot of monitoring going on in the number of interventions but I think it comes back to the whole picture again – we have an ageing population with an increasing number of illnesses that need to be dealt with.
Porter Do you know for sure that your gateways, if you like, to limit the treatments that are being done, to prioritise the treatments that are being done, actually work in terms of cost effectiveness, that they’re saving your CCG money?
Jackson I think there is monitoring within the system and clearly there’s a cost for those gateways and we have to be honest there is a cost to run those gateways and it’s important that those costs are monitored against the cost of procedures.
Porter Because it might be that a particular gateway that’s put in with all the best intentions might end up not working, it might not be cost effective to do that but to make that decision you need to be monitoring these very closely and that is going on is it across the country?
Jackson It is going on and then there is clearly – everything we do has a cost attached to it and the basic premise is that we have limited resource and we must not squander that resource.
Porter Yes I mean we mustn’t squander it on unnecessary treatments but we mustn’t squander it on unnecessary admin but we’re looking at the treatments from an evidence base – I mean I’m just asking are we applying those same stringent rules to the gateway interventions, to the admin behind this?
Jackson The gateway interventions are monitored monetarily but also from a quality perspective to make sure they do provide the quality assessment that we need.
Porter Dr Graham Jackson. So given that CCGs across England are monitoring the impact of prioritising treatments like hernia repairs, and hand and varicose vein surgery, we went looking for published examples of their findings. When I say we….
McCartney Mark, I may never forgive you for this. I’ve spent the last week trawling through minutes from CCGs looking to see who is looking at the harms of the procedures that people have put in place to try and limit access to interventions. I can find almost none. I can find people that have written down things like – Will this affect people, for example, older people more or carers more, qualities analysis, but I cannot find any analysis done of the cost effectiveness of the entire procedure.
Porter Well Graham says it’s being monitored, so one would imagine that if his CCG’s doing that that that’s happening across the country but what you’re saying is that nothing is being published?
McCartney I can’t find anything in the public domain, if any listeners know of any please do send it in for me. And of course there’s all sorts of other costs associated with not doing things, for example people having more physiotherapy, people attending their GP more to get painkillers, people being off work, people maybe needing to see a psychologist, people not being able to care for family or relatives. These costs, I think, are being absorbed elsewhere into the system and they’re not being properly tabulated.
Porter And of course the other aspect is the cost of the bureaucracy itself, which needs to be balanced against the cost of not doing some of these operations.
McCartney Yeah, ask GPs how much time they’re spending doing paperwork as opposed to face to face patient care – it’s huge and it’s growing and I don’t think anyone’s really got a clear handle on how much of this is being generated by CCGs and these type of rules.
Porter But we can’t be dismissive of it because we don’t know because the evidence isn’t published?
McCartney And that’s a big problem, whenever you’re putting a new policy into practice I think it should be incumbent on the policymakers to say what are the potential harms, what are the potential downsides and how are we going to find out about them because if you don’t look for them you will not find them, they will be buried and they’ll just come back to bite you on the posterior later on.
Porter Margaret McCartney – who will be one of the panellists in our upcoming hour long special debate on the NHS – what needs to give? – which will be aired on Valentine’s day. In the meantime normal service resumes next week when I will learning how virtual reality is being used to help people with conditions as diverse as Alzheimer’s disease and phantom limb pain. As well as taking a closer look at the latest initiative to limit and target antibiotic use for sore throats.
ENDSTHE ATTACHED TRANSCRIPT WAS TYPED FROM A RECORDING AND NOT COPIED FROM AN ORIGINAL SCRIPT. BECAUSE OF THE RISK OF MISHEARING AND THE DIFFICULTY IN SOME CASES OF IDENTIFYING INDIVIDUAL SPEAKERS, THE BBC CANNOT VOUCH FOR ITS COMPLETE ACCURACY.
INSIDE HEALTH
Programme 5.
TX: 31.01.17 2100-2130
PRESENTER: MARK PORTER
PRODUCER: ERIKA WRIGHT
Porter Coming up today carpal tunnel syndrome, hernias and varicose veins and why you might now struggle to get any of them treated on the NHS.
And the difficulty is not limited to these common complaints. Clinical Commissioning Groups in the Midlands have been in the headlines this week after raising the bar for eligibility for hip and knee replacements. If you live in Worcestershire your arthritis now needs to be severe enough to cause pain that interferes with daily life and keeps you awake at night. If it’s not then the local CCGs won’t pay for the surgery. A move they believe will lead to 350 fewer operations, saving them around £20 million a year to spend on other therapies they deem higher priority.
Prioritisation is otherwise known as rationing and there’s a burgeoning number of interventions on the not normally funded list, produced by CCGs to show what they are not prepared to pay for unless there are exceptional circumstances.
Clinicians with patients they regard as special cases with things like hernias have to seek approval using an individual funding request – or IFR – which is appraised by a panel to check the patient meets the necessary criteria.
Jonothan Earnshaw is Consultant Surgeon at Cheltenham General Hospital.
Earnshaw Groin hernias are very common and the danger with having a groin hernia is strangulation where a piece of bowel gets into the hernia and twists and in that circumstance people need an urgent hernia repair and sometimes even the bowel needs to be removed. And the reason for doing routine elective hernia repair is to prevent strangulation. The problem is it’s really very tricky to assess whether an individual hernia is likely to strangulate and for that reason we’ve ended up in the past operating on most people who have hernias, unless there was a strong reason not to – if someone was very elderly or unfit and very occasionally I suppose we wouldn’t treat minor, small hernias – but essentially all people with hernias had surgery for them.
Porter So fast forward to today, what’s the situation now?
Earnshaw Well over the last 10 years we’ve certainly had various different protocols that have been given to us to try and reduce the number of hernias that we operate on. Sometimes we’ve been asked to mend just painful ones or sometimes we’ve been asked mend only ones that are likely to strangulate but that’s a very non-specific way of being able to tell the difference between hernias and that’s not very helpful for me to decide whether or not to fix them.
Porter And the driver behind that has been what – the clinical evidence base that shows that some hernias don’t need treating, won’t cause trouble or is it mainly a cost issue?
Earnshaw The main driver, as with so many of these things, is cost, to reduce the number of hernias that are done that really are never going to strangulate. The science shows actually that if you take people with small hernias and there have been a couple of randomised trials where people either operate on a hernia or select patients for watchful waiting and see what happens over a number of years and if you do that over about 10 years most of the watchful waiting group get bigger and need surgery.
Porter So you might be delaying the inevitable with a lot of these patients?
Earnshaw I think that’s exactly what you’re doing.
Porter But what’s practically involved as a consultant? So I see somebody with a common type of hernia, I send them to you, you then look at them and say I think this needs an operation – what happens?
Earnshaw So at the moment the rules have changed. A couple of years ago we all had to fill a form in which was sent to the interventions not normally funded group and they checked the forms to see whether they matched criteria for surgery.
Porter So this was even though you decided that the patient needed surgery, somebody else is checking that…?
Earnshaw Was checking it, yes, and turning some of them down, saying that they weren’t suitable for repair, particularly those who had direct more mild hernias, if my clinic letter didn’t say that they had severe pain then they were often turned down.
Porter So severe pain being one of the boxes you had to tick.
Earnshaw Being one of the boxes, absolutely and in a working age person having a hernia, particularly if you’ve got a manual job, can be very uncomfortable.
Porter So are you spending a lot of your time now filling in these funding referrals for hernias?
Earnshaw No that seems to have stopped and I’ve assumed that the Clinical Commissioning Groups have found that it actually doesn’t reduce the number of people who get operations and therefore that the costs of this layer of bureaucracy actually aren’t worth it.
Porter So essentially it might have been that it was an administrative hurdle that wasn’t actually making a lot of difference.
Earnshaw Exactly right.
Porter How does your practice here compare to practices elsewhere in the country? Are you operating on a similar proportion of the hernias that you see?
Earnshaw No, my colleagues around the country tell me that there’s a very big discrepancy between who gets hernia repairs. In some places, like Gloucestershire, it’s pretty easy to get your hernia repaired if there is an appropriate reason for doing so.
Porter So that’s your decision.
Earnshaw So that’s my decision. What happens for that is that because people are able to travel is they often come over here to get their hernia repaired from neighbouring counties. In many parts of the country it’s extraordinarily difficult to get your hernia repaired and the difficulty of course is to assess which hernias are the ones which are most likely to strangulate, it’s a very difficult clinical decision.
Porter But it must be that your colleagues in other parts of the country are wanting to operate on the ones that they think might strangulate, so are they better or worse at selecting them than you or is it an inexact science?
Earnshaw It’s a very inexact science and I think it must be deeply frustrating to find that you can only operate on a very small proportion of people with hernias because hernias are uncomfortable and it’s one of the operations I do that people seem to derive most benefit from in terms of improving their symptoms.
Porter And if you’re not operating on many people you will, be default, miss some that go on to strangulate.
Earnshaw Yes and I would imagine that in areas where you don’t do a lot of elective hernia repairs you will start to see people with strangulated hernias. And fixing a strangulate hernia in an emergency is not an easy thing to do.
Porter Surgeon Jonothan Earnshaw.
Inside Health’s Margaret McCartney has been looking at what research says about the impact of limiting access to treatments like hernia surgery.
McCartney Mark, I have found the evidence, it’s taken me the best part of a week, but I can back this up. In 2009 the Department of Health had asked the management consultancy McKinsey to find out how to make services more cost effective in England and one of the things they proposed was that groin hernias in the main didn’t have to be operated on because mainly people got on just as well if they didn’t have an operation than if they did. And this was proposed as a cost saving device and as a result many CCGs decided to no longer operate routinely for people who had groin hernias that didn’t seem to be causing them much problem. And that might seem on one level absolutely fine, why interfere with something that wasn’t causing you problems anyway? But at that time no one had investigated what the consequences of this new policy would be. Well a group of surgeons went and looked to see what happened in the 16 months before and after this new policy. And what they found was that this policy change made more people who had a hernia, that hadn’t been operated on, end up turning up as an emergency, needing an emergency procedure done on that hernia that had then developed a problem.
Porter And in terms of numbers what sort of numbers are we talking about?
McCartney Overall it’s still small, so this is not to needlessly alarm people who decided on the basis of a discussion with their doctors or healthcare provider not to have surgery. But what these doctors found that was pretty much a doubling of people needing emergency repairs who hadn’t had the operation done, that was 3.6% versus 5.5%. And what was really important was the people in that group who did need emergency care tended to have more adverse effects, more problems after the surgery compared with people who’d had it done routinely. That’s the big problem.
Porter Knowing how cynical our Inside Health audience is I suppose my next question should be – well surgeons would say that wouldn’t they?
McCartney Mark, I like the cynicism, I support cynicism myself but this was just number counting, this was just looking at what happened afterwards. So I think in this study there was a limited chance of bias.
Porter So we’re looking at something like just under one in 20 people needing to have emergency surgery, if – if they were left.
McCartney Yeah, now we can’t prove cause and effect, this wasn’t a randomised control trial, it was a study looking at the association of a new policy but it’s the best data we have and that is flagging up a problem. Now it’s completely different if people are sitting down talking about what to do about a problem and making a valid decision based on individual judgement about a set of circumstances. The big problem is that McKinsey, who made the recommendation not to routinely operate on people with inguinal hernias, they based this policy on trials that were done from America, but the trials are flawed when we start to compare with them with practice in the UK of enforcing this policy because over half the people offered entry into the trials didn’t take part in it, they declined to do so, they wanted to have surgery anyway. So we cannot compare like with like, we cannot say that therefore this policy is going to benefit our patients in the UK, the data was flawed.
Porter So the findings of the research might have been skewed by the people who were included in the trial but you’re confident that this second trial, where the surgeons went to look to see what happened to these people, that that was reflective of real life practice?
McCartney Well this is real life practice, it’s not a clinical trial, we can’t prove cause and effect but we certainly can say that this policy was associated with a change in the amount of people who presented as an emergency.
Porter Margaret McCartney.
Hand surgery is another area that has been targeted by CCGs looking to save resources. Ash Merry’s specialist had to apply for funding when he felt she needed surgery for carpal tunnel syndrome – a common complaint caused by entrapment of one of the nerves supplying the hand. And it was giving her a lot of trouble.
Merry Pins and needles. Not during the day but specifically at night. And I used to lie in bed, put my hands above my head and I was kept awake literally by the pain in my right hand and it is excruciating, it’s like electric shocks going up and down your arm and you cannot stop it. It was quite literally wrecking my life I felt.
Porter And how long had that been going on before you first sought medical advice?
Merry Not sleeping at night, it has been going on intermittently probably for about a year.
Porter So you went to see your doctor?
Merry Yes. I went to see the doctor in March 2016 and I went to see a consultant before Christmas and I thought ooh this is to check yes what surgery’s going to be. No it wasn’t. We have to now apply for funding.
Porter Had you ever heard of anything like this happening before?
Merry No, I jolly well hadn’t.
Pailthorpe So I’m Charles Pailthorpe, I’m a Consultant Orthopaedic Surgeon with a specialist interest in the hand at the Royal Berkshire Hospital in Reading. My practice as a hand surgeon has changed quite dramatically over the past couple of years with the individual funding requests policy. It’s become almost an administrative nightmare, having to spend more and more time filling in forms, I don’t think it’s got any benefit to my patients at all. And the problem in hand surgery is that it affects almost half my practice, so simple, in relative terms, conditions called carpal tunnel syndrome, which is a trapped nerve, things like a trigger finger where the finger gets caught and a condition called Dupuytren’s where the finger actually gets stuck – these are common hand conditions but now have to have funding requested. CCGs have stated in their funding request information that exceptional health requirement is over and above what is there for the general public. But if you’ve got a condition that’s affecting your life and stopping you either from sleeping, like carpal tunnel syndrome or you’re unable to do your job because you can’t feel your hands and you’re dropping things why is that exceptional above the general public? It’s not and so this rationing purposes doesn’t take into effect what’s happening to the actual patient themselves.
And so from my perspective my job is to treat the patient and each patient who uses their hands is individual, we’re all individuals, we all use our hands, we all abuse our hands but we all do it differently. So what is a problem for one person isn’t for somebody else. And so actually having a checklist of so-called interventions before you can do surgery doesn’t make sense for an individual where there may well be exceptional reasons. So I’m having my professional integrity in essence questioned by having to prove exceptional health requirements.
Porter Is that part of it though, I mean that you feel that you’re being undermined professionally, I mean is that one of the reasons that I mean it gets your goat, I can feel it?
Pailthorpe You know I’ve been a hand surgeon since 1995, I think I’m not a knife happy surgeon, I’m a very cautious surgeon but when I do make a decision with the patient’s agreement that surgery’s appropriate I’d like to feel that I have the professional integrity that that’s correct.
Porter Looking at carpal tunnel syndrome, it’s a common problem, we see a lot of it in general practice, refer a lot of it to surgeons like you, how many of the patients that you feel definitely need an operation do you get approved easily or are you constantly getting refusals?
Pailthorpe We think that we’re probably getting about a 20% rejection rate and that’s largely based on a failure of the checklist concept. So if they haven’t had a splint or if they haven’t had an injection it’s often rejected, they say why haven’t they had an injection, despite the fact that I’ve put down sometimes the reason why I think an injection’s not appropriate, because there are sometimes reasons, they’ve still be rejected.
Porter Because that’s the other part of the rationalisation isn’t it, it’s not just about saving resources but it’s using resources appropriately and getting people to follow guidelines. So for instance with carpal tunnel they might get somebody like me to say we’ll try a splint for four to six weeks first, then refer to you, you might consider an injection and then surgery as a last resort.
Pailthorpe Well I don’t have a problem with that actually but there are exceptions. What we haven’t got at the moment is a way of agreeing those exceptions with the clinical groups. For example, in carpal tunnel syndrome if somebody’s got wasting of their thumb muscles that should be just let through, we shouldn’t have to apply for funding.
Porter They need an operation.
Pailthorpe Yeah, they need an operation, it’s a barn door decision, you just need to get on and get it done sort of thing.
Merry I have paid contributions for 37 years, I can understand that good housekeeping is vital, however, when it comes to something like carpal tunnel surgery, as I understand it, when it is severe whatever you do to it at some stage surgery is going to be needed. To stop the progression of impairment in your dominant hand I would argue that any delay could be more costly to the NHS.
Porter So what happened in your case?
Merry Well what happened in my case is I have to say I made a bit of a noise. I was constantly chasing it. So when funding was approved the process was really remarkably quick. I’ve since found out there are vacant surgery slots that are not being filled with staff on standby, which is costing money, that are going vacant because they were waiting for funding requests to be approved.
Pailthorpe To me it’s almost as if some days they’ve used their quota up because it seems to be completely irrational – other ones go through without a problem and then I’ll get one rejected.
Porter What happens to those 20% of patients, what’s the risk of not operating on somebody like Ash?
Pailthorpe Well the risk in her case in fact is that the pressure on the nerve cause permanent damage.
Porter So looking at those 20% that are refused are any of them ever going to get better on their own or are they going to end up under your care having an operation at some stage?
Pailthorpe I don’t think it ever goes. The trouble is that the literature is confusing sometimes when it comes to certain treatments, particularly when it comes to simple things like carpal tunnel because sometimes there isn’t an awful lot of evidence but there’s an awful lot of common sense and experience.
Porter Because this is one of the areas that the people behind these criteria will say look there isn’t enough evidence to support this intervention and what you’re saying is it’s just because there isn’t enough evidence. It might be that the trials haven’t been done, it’s not that the procedure doesn’t work – is that what you’re saying?
Pailthorpe Yeah to a certain extent yes. Though there is, I think, more evidence coming out. There is a big study in fact in Sweden on corticosteroid injections and showed that again in certain specific instances is actually a very effective treatment and will reduce the symptoms for a year or more, though…
Porter But is it delaying the inevitable?
Pailthorpe They eventually all still come to surgery at some point because nobody has followed them up for another 10 years. And so that’s why the evidence is fundamentally flawed and I do have some patients who grumble along for years, have had some ladies who’ve come to me in their 50s, 60s and said well I’ve had it for 20 years but now actually I can’t feel my fingers. Well it’s almost too late then. So there comes a time where actually there is an opportune time to get on with it.
Porter What’s happening in other parts of the country, is this something that’s happening pretty uniformly?
Pailthorpe No I don’t think so, it seems to me that there are – some of my colleagues I’ve chatted to they say well what are IFRs – individual funding requests – they don’t have to do them. So some parts of the country it’s not active at the moment but other parts it’s obviously almost draconian.
Porter Ash mentioned empty slots where because the funding’s not coming through there’s a slot that could have been used but the team’s all still there, is that actually happening?
Pailthorpe Yes. We were planning to do a list at the end of January and we have something I think in the region of 40-50 patients where we’re waiting on funding. So it was all set to go but we just haven’t got the patients at the moment to fill the list. Overall there’s a lot of waste of money in this process. We’ve had to employ an administrative staff just for IFRs!
Porter Charles Pailthorpe and his patient Ash Merry.
Back in Cheltenham surgeon Jonothan Earnshaw treats varicose veins as well as hernias, and he too has witnessed a dramatic change in practice over recent years. His team now does half the operations it used to.
Earnshaw Over the years there’s been an increasing thought that in fact a lot of varicose veins don’t need to be done – they’re either cosmetic or there’s no medical advantage in doing them – and so we’ve had great restrictions on the sort of veins that we can treat. So we tend now only to be allowed to treat people who’ve got complications from their veins, not just simple discomfort.
Porter And the sort of complications that you’d have to have – the boxes that you’d have to tick – to get approved for your surgery would be what?
Earnshaw So if you have varicose veins long enough they start to affect the skin around your ankle and you’ve seen the brown speckling there which is called varicose eczema and that’s a sign that there’s high pressure in the veins of the skin. If you don’t treat people with varicose eczema there’s a high chance if they damage their skin they will get a varicose ulcer and varicose ulcers are common particularly in the elderly. So the idea of treating people with varicose veins is to prevent them getting the complications of varicose ulcer.
Porter And presumably once somebody develops that complication that’s expensive and difficult to deal with?
Earnshaw Oh yes and painful, it’s horrible having a varicose ulcer, it really grossly affects quality of life. And most of the guidelines and restrictions on treatment for varicose veins allow treatment of people with complicated varicose veins for that very reason. And the guidelines for varicose veins are much easier because the classification of varicose veins is easier. It’s obvious when people are starting to get complications in their veins – and those are the ones we treat – it’s obvious which are the ones don’t have complications and those generally speaking are the ones that we don’t treat.
Porter Are you happy with where the bar is set?
Earnshaw Well again the bar is very variable around the country. Here in Gloucestershire we’re allowed to treat people with complicated varicose veins and people whose varicose veins severely affect their quality of life. The problem of course is who decides whether a quality of life is severely affected and we often end up having quite uncomfortable consultations in outpatients where perhaps my perception of quality of life isn’t quite the same as the person who has their varicose veins and that can lead to considerable difficulty.
Porter So will you sometimes tell a patient in outpatients look you’re not going to meet the threshold, we’re not going to be able to operate on you or we don’t need to operate on you?
Earnshaw That happens in every clinic that I do. We have people who come with what they regard as severe symptoms from their varicose veins but actually when you question them they’re not affecting their sleep, they don’t require painkillers, they’re not actually affecting their work and under those circumstances our local commissioning wouldn’t fund that intervention. So I have to tell patients then that I can’t operate on their veins.
Porter But what happens to them if you don’t operate on their veins, I mean they’re not going to get better are they, I mean presumably with time they get worse – do they – are we just delaying the inevitable here as well?
Earnshaw Well that’s not quite the case because as a GP you’ll have had many patients who have varicose veins for years and years and years and years and years that never ever get any complications and if we could predict which people with varicose veins were going to go on and get complications then it would be easy to select those out but we can’t and most people don’t get complications from their varicose veins. So there are reasonable medicine reasons for not operating, not treating people with varicose veins, until they actually start to get the complications.
Porter So what might happen is a patient might be referred into you, you say don’t need to operate, or can’t operate now, come back when you’ve got a complication for those that do?
Earnshaw Exactly right and as a surgeon who’s been in one place for a very long time that happens not infrequently. But of course the corollary of that is that I’ve sent away a lot of people and reassured them their veins are no threat to their health and they’ve never come back over the years.
Porter Jonothan Earnshaw.
Clinical Commissioning Groups - CCGs - are in a difficult position, squeezed between the expectations of their public and the demands of their doctors and other healthcare professionals.
Buckinghamshire GP Graham Jackson is Chair of his local CCG, and co-Chair of NHS Clinical Commissioners.
Jackson Clinical Commissioning Groups are allocated a certain amount of resource from central government to spend on healthcare in their locality or their area. And what we have to do is decide how to spend that resource most effectively. Cancer services, emergency services, surgical interventions – and so we have to make decisions based on the population and remembering the populations differ from different parts of the country and then how we spend that money is based on their local need.
Porter And put simply, if you spend more money on people having minor varicose veins treated, for instance, that leaves you less money to help people who might have severe arthritis and require a hip replacement?
Jackson Well it’s certainly true there’s only a finite fixed amount of fund.
Porter One of the criticisms aimed at the current set up is that there’s something of what’s become known as the postcode lottery, that if the criteria for all of these procedures, for getting your hand surgery done, your varicose veins done or your hip done was the same in every area of the country and people understand there are limited resources then perhaps everyone would buy into it much more. Why is there this variability?
Jackson I think the variability comes back to the fact that we are locally focused and so the priorities for spending healthcare in a particular area need to be matched to the priority of that population and it’s really important to understand that the local population has different needs from different parts of the country, even actually in say the same county in different areas based on their age profile etc.
Porter And are some CCGs under more financial pressures than others because of that change in demography?
Jackson I think that is true. There is an allocation across the country from CCG to CCG based on that profile but it’s very difficult to make those allocations absolutely accurate everywhere.
Porter One of the concerns, I suppose, is that we are delaying the inevitable, so that by reducing perhaps the number of hernias that we operate on we end up maybe with more people coming in with strangulations that are expensive and obviously have implications for the patient. I presume we’re monitoring this situation ongoing to check that these interventions are cost effective in the long term?
Jackson Yes there’s a lot of monitoring going on in the number of interventions but I think it comes back to the whole picture again – we have an ageing population with an increasing number of illnesses that need to be dealt with.
Porter Do you know for sure that your gateways, if you like, to limit the treatments that are being done, to prioritise the treatments that are being done, actually work in terms of cost effectiveness, that they’re saving your CCG money?
Jackson I think there is monitoring within the system and clearly there’s a cost for those gateways and we have to be honest there is a cost to run those gateways and it’s important that those costs are monitored against the cost of procedures.
Porter Because it might be that a particular gateway that’s put in with all the best intentions might end up not working, it might not be cost effective to do that but to make that decision you need to be monitoring these very closely and that is going on is it across the country?
Jackson It is going on and then there is clearly – everything we do has a cost attached to it and the basic premise is that we have limited resource and we must not squander that resource.
Porter Yes I mean we mustn’t squander it on unnecessary treatments but we mustn’t squander it on unnecessary admin but we’re looking at the treatments from an evidence base – I mean I’m just asking are we applying those same stringent rules to the gateway interventions, to the admin behind this?
Jackson The gateway interventions are monitored monetarily but also from a quality perspective to make sure they do provide the quality assessment that we need.
Porter Dr Graham Jackson. So given that CCGs across England are monitoring the impact of prioritising treatments like hernia repairs, and hand and varicose vein surgery, we went looking for published examples of their findings. When I say we….
McCartney Mark, I may never forgive you for this. I’ve spent the last week trawling through minutes from CCGs looking to see who is looking at the harms of the procedures that people have put in place to try and limit access to interventions. I can find almost none. I can find people that have written down things like – Will this affect people, for example, older people more or carers more, qualities analysis, but I cannot find any analysis done of the cost effectiveness of the entire procedure.
Porter Well Graham says it’s being monitored, so one would imagine that if his CCG’s doing that that that’s happening across the country but what you’re saying is that nothing is being published?
McCartney I can’t find anything in the public domain, if any listeners know of any please do send it in for me. And of course there’s all sorts of other costs associated with not doing things, for example people having more physiotherapy, people attending their GP more to get painkillers, people being off work, people maybe needing to see a psychologist, people not being able to care for family or relatives. These costs, I think, are being absorbed elsewhere into the system and they’re not being properly tabulated.
Porter And of course the other aspect is the cost of the bureaucracy itself, which needs to be balanced against the cost of not doing some of these operations.
McCartney Yeah, ask GPs how much time they’re spending doing paperwork as opposed to face to face patient care – it’s huge and it’s growing and I don’t think anyone’s really got a clear handle on how much of this is being generated by CCGs and these type of rules.
Porter But we can’t be dismissive of it because we don’t know because the evidence isn’t published?
McCartney And that’s a big problem, whenever you’re putting a new policy into practice I think it should be incumbent on the policymakers to say what are the potential harms, what are the potential downsides and how are we going to find out about them because if you don’t look for them you will not find them, they will be buried and they’ll just come back to bite you on the posterior later on.
Porter Margaret McCartney – who will be one of the panellists in our upcoming hour long special debate on the NHS – what needs to give? – which will be aired on Valentine’s day. In the meantime normal service resumes next week when I will learning how virtual reality is being used to help people with conditions as diverse as Alzheimer’s disease and phantom limb pain. As well as taking a closer look at the latest initiative to limit and target antibiotic use for sore throats.
ENDSTHE ATTACHED TRANSCRIPT WAS TYPED FROM A RECORDING AND NOT COPIED FROM AN ORIGINAL SCRIPT. BECAUSE OF THE RISK OF MISHEARING AND THE DIFFICULTY IN SOME CASES OF IDENTIFYING INDIVIDUAL SPEAKERS, THE BBC CANNOT VOUCH FOR ITS COMPLETE ACCURACY.
INSIDE HEALTH
Programme 5.
TX: 31.01.17 2100-2130
PRESENTER: MARK PORTER
PRODUCER: ERIKA WRIGHT
Porter Coming up today carpal tunnel syndrome, hernias and varicose veins and why you might now struggle to get any of them treated on the NHS.
And the difficulty is not limited to these common complaints. Clinical Commissioning Groups in the Midlands have been in the headlines this week after raising the bar for eligibility for hip and knee replacements. If you live in Worcestershire your arthritis now needs to be severe enough to cause pain that interferes with daily life and keeps you awake at night. If it’s not then the local CCGs won’t pay for the surgery. A move they believe will lead to 350 fewer operations, saving them around £20 million a year to spend on other therapies they deem higher priority.
Prioritisation is otherwise known as rationing and there’s a burgeoning number of interventions on the not normally funded list, produced by CCGs to show what they are not prepared to pay for unless there are exceptional circumstances.
Clinicians with patients they regard as special cases with things like hernias have to seek approval using an individual funding request – or IFR – which is appraised by a panel to check the patient meets the necessary criteria.
Jonothan Earnshaw is Consultant Surgeon at Cheltenham General Hospital.
Earnshaw Groin hernias are very common and the danger with having a groin hernia is strangulation where a piece of bowel gets into the hernia and twists and in that circumstance people need an urgent hernia repair and sometimes even the bowel needs to be removed. And the reason for doing routine elective hernia repair is to prevent strangulation. The problem is it’s really very tricky to assess whether an individual hernia is likely to strangulate and for that reason we’ve ended up in the past operating on most people who have hernias, unless there was a strong reason not to – if someone was very elderly or unfit and very occasionally I suppose we wouldn’t treat minor, small hernias – but essentially all people with hernias had surgery for them.
Porter So fast forward to today, what’s the situation now?
Earnshaw Well over the last 10 years we’ve certainly had various different protocols that have been given to us to try and reduce the number of hernias that we operate on. Sometimes we’ve been asked to mend just painful ones or sometimes we’ve been asked mend only ones that are likely to strangulate but that’s a very non-specific way of being able to tell the difference between hernias and that’s not very helpful for me to decide whether or not to fix them.
Porter And the driver behind that has been what – the clinical evidence base that shows that some hernias don’t need treating, won’t cause trouble or is it mainly a cost issue?
Earnshaw The main driver, as with so many of these things, is cost, to reduce the number of hernias that are done that really are never going to strangulate. The science shows actually that if you take people with small hernias and there have been a couple of randomised trials where people either operate on a hernia or select patients for watchful waiting and see what happens over a number of years and if you do that over about 10 years most of the watchful waiting group get bigger and need surgery.
Porter So you might be delaying the inevitable with a lot of these patients?
Earnshaw I think that’s exactly what you’re doing.
Porter But what’s practically involved as a consultant? So I see somebody with a common type of hernia, I send them to you, you then look at them and say I think this needs an operation – what happens?
Earnshaw So at the moment the rules have changed. A couple of years ago we all had to fill a form in which was sent to the interventions not normally funded group and they checked the forms to see whether they matched criteria for surgery.
Porter So this was even though you decided that the patient needed surgery, somebody else is checking that…?
Earnshaw Was checking it, yes, and turning some of them down, saying that they weren’t suitable for repair, particularly those who had direct more mild hernias, if my clinic letter didn’t say that they had severe pain then they were often turned down.
Porter So severe pain being one of the boxes you had to tick.
Earnshaw Being one of the boxes, absolutely and in a working age person having a hernia, particularly if you’ve got a manual job, can be very uncomfortable.
Porter So are you spending a lot of your time now filling in these funding referrals for hernias?
Earnshaw No that seems to have stopped and I’ve assumed that the Clinical Commissioning Groups have found that it actually doesn’t reduce the number of people who get operations and therefore that the costs of this layer of bureaucracy actually aren’t worth it.
Porter So essentially it might have been that it was an administrative hurdle that wasn’t actually making a lot of difference.
Earnshaw Exactly right.
Porter How does your practice here compare to practices elsewhere in the country? Are you operating on a similar proportion of the hernias that you see?
Earnshaw No, my colleagues around the country tell me that there’s a very big discrepancy between who gets hernia repairs. In some places, like Gloucestershire, it’s pretty easy to get your hernia repaired if there is an appropriate reason for doing so.
Porter So that’s your decision.
Earnshaw So that’s my decision. What happens for that is that because people are able to travel is they often come over here to get their hernia repaired from neighbouring counties. In many parts of the country it’s extraordinarily difficult to get your hernia repaired and the difficulty of course is to assess which hernias are the ones which are most likely to strangulate, it’s a very difficult clinical decision.
Porter But it must be that your colleagues in other parts of the country are wanting to operate on the ones that they think might strangulate, so are they better or worse at selecting them than you or is it an inexact science?
Earnshaw It’s a very inexact science and I think it must be deeply frustrating to find that you can only operate on a very small proportion of people with hernias because hernias are uncomfortable and it’s one of the operations I do that people seem to derive most benefit from in terms of improving their symptoms.
Porter And if you’re not operating on many people you will, be default, miss some that go on to strangulate.
Earnshaw Yes and I would imagine that in areas where you don’t do a lot of elective hernia repairs you will start to see people with strangulated hernias. And fixing a strangulate hernia in an emergency is not an easy thing to do.
Porter Surgeon Jonothan Earnshaw.
Inside Health’s Margaret McCartney has been looking at what research says about the impact of limiting access to treatments like hernia surgery.
McCartney Mark, I have found the evidence, it’s taken me the best part of a week, but I can back this up. In 2009 the Department of Health had asked the management consultancy McKinsey to find out how to make services more cost effective in England and one of the things they proposed was that groin hernias in the main didn’t have to be operated on because mainly people got on just as well if they didn’t have an operation than if they did. And this was proposed as a cost saving device and as a result many CCGs decided to no longer operate routinely for people who had groin hernias that didn’t seem to be causing them much problem. And that might seem on one level absolutely fine, why interfere with something that wasn’t causing you problems anyway? But at that time no one had investigated what the consequences of this new policy would be. Well a group of surgeons went and looked to see what happened in the 16 months before and after this new policy. And what they found was that this policy change made more people who had a hernia, that hadn’t been operated on, end up turning up as an emergency, needing an emergency procedure done on that hernia that had then developed a problem.
Porter And in terms of numbers what sort of numbers are we talking about?
McCartney Overall it’s still small, so this is not to needlessly alarm people who decided on the basis of a discussion with their doctors or healthcare provider not to have surgery. But what these doctors found that was pretty much a doubling of people needing emergency repairs who hadn’t had the operation done, that was 3.6% versus 5.5%. And what was really important was the people in that group who did need emergency care tended to have more adverse effects, more problems after the surgery compared with people who’d had it done routinely. That’s the big problem.
Porter Knowing how cynical our Inside Health audience is I suppose my next question should be – well surgeons would say that wouldn’t they?
McCartney Mark, I like the cynicism, I support cynicism myself but this was just number counting, this was just looking at what happened afterwards. So I think in this study there was a limited chance of bias.
Porter So we’re looking at something like just under one in 20 people needing to have emergency surgery, if – if they were left.
McCartney Yeah, now we can’t prove cause and effect, this wasn’t a randomised control trial, it was a study looking at the association of a new policy but it’s the best data we have and that is flagging up a problem. Now it’s completely different if people are sitting down talking about what to do about a problem and making a valid decision based on individual judgement about a set of circumstances. The big problem is that McKinsey, who made the recommendation not to routinely operate on people with inguinal hernias, they based this policy on trials that were done from America, but the trials are flawed when we start to compare with them with practice in the UK of enforcing this policy because over half the people offered entry into the trials didn’t take part in it, they declined to do so, they wanted to have surgery anyway. So we cannot compare like with like, we cannot say that therefore this policy is going to benefit our patients in the UK, the data was flawed.
Porter So the findings of the research might have been skewed by the people who were included in the trial but you’re confident that this second trial, where the surgeons went to look to see what happened to these people, that that was reflective of real life practice?
McCartney Well this is real life practice, it’s not a clinical trial, we can’t prove cause and effect but we certainly can say that this policy was associated with a change in the amount of people who presented as an emergency.
Porter Margaret McCartney.
Hand surgery is another area that has been targeted by CCGs looking to save resources. Ash Merry’s specialist had to apply for funding when he felt she needed surgery for carpal tunnel syndrome – a common complaint caused by entrapment of one of the nerves supplying the hand. And it was giving her a lot of trouble.
Merry Pins and needles. Not during the day but specifically at night. And I used to lie in bed, put my hands above my head and I was kept awake literally by the pain in my right hand and it is excruciating, it’s like electric shocks going up and down your arm and you cannot stop it. It was quite literally wrecking my life I felt.
Porter And how long had that been going on before you first sought medical advice?
Merry Not sleeping at night, it has been going on intermittently probably for about a year.
Porter So you went to see your doctor?
Merry Yes. I went to see the doctor in March 2016 and I went to see a consultant before Christmas and I thought ooh this is to check yes what surgery’s going to be. No it wasn’t. We have to now apply for funding.
Porter Had you ever heard of anything like this happening before?
Merry No, I jolly well hadn’t.
Pailthorpe So I’m Charles Pailthorpe, I’m a Consultant Orthopaedic Surgeon with a specialist interest in the hand at the Royal Berkshire Hospital in Reading. My practice as a hand surgeon has changed quite dramatically over the past couple of years with the individual funding requests policy. It’s become almost an administrative nightmare, having to spend more and more time filling in forms, I don’t think it’s got any benefit to my patients at all. And the problem in hand surgery is that it affects almost half my practice, so simple, in relative terms, conditions called carpal tunnel syndrome, which is a trapped nerve, things like a trigger finger where the finger gets caught and a condition called Dupuytren’s where the finger actually gets stuck – these are common hand conditions but now have to have funding requested. CCGs have stated in their funding request information that exceptional health requirement is over and above what is there for the general public. But if you’ve got a condition that’s affecting your life and stopping you either from sleeping, like carpal tunnel syndrome or you’re unable to do your job because you can’t feel your hands and you’re dropping things why is that exceptional above the general public? It’s not and so this rationing purposes doesn’t take into effect what’s happening to the actual patient themselves.
And so from my perspective my job is to treat the patient and each patient who uses their hands is individual, we’re all individuals, we all use our hands, we all abuse our hands but we all do it differently. So what is a problem for one person isn’t for somebody else. And so actually having a checklist of so-called interventions before you can do surgery doesn’t make sense for an individual where there may well be exceptional reasons. So I’m having my professional integrity in essence questioned by having to prove exceptional health requirements.
Porter Is that part of it though, I mean that you feel that you’re being undermined professionally, I mean is that one of the reasons that I mean it gets your goat, I can feel it?
Pailthorpe You know I’ve been a hand surgeon since 1995, I think I’m not a knife happy surgeon, I’m a very cautious surgeon but when I do make a decision with the patient’s agreement that surgery’s appropriate I’d like to feel that I have the professional integrity that that’s correct.
Porter Looking at carpal tunnel syndrome, it’s a common problem, we see a lot of it in general practice, refer a lot of it to surgeons like you, how many of the patients that you feel definitely need an operation do you get approved easily or are you constantly getting refusals?
Pailthorpe We think that we’re probably getting about a 20% rejection rate and that’s largely based on a failure of the checklist concept. So if they haven’t had a splint or if they haven’t had an injection it’s often rejected, they say why haven’t they had an injection, despite the fact that I’ve put down sometimes the reason why I think an injection’s not appropriate, because there are sometimes reasons, they’ve still be rejected.
Porter Because that’s the other part of the rationalisation isn’t it, it’s not just about saving resources but it’s using resources appropriately and getting people to follow guidelines. So for instance with carpal tunnel they might get somebody like me to say we’ll try a splint for four to six weeks first, then refer to you, you might consider an injection and then surgery as a last resort.
Pailthorpe Well I don’t have a problem with that actually but there are exceptions. What we haven’t got at the moment is a way of agreeing those exceptions with the clinical groups. For example, in carpal tunnel syndrome if somebody’s got wasting of their thumb muscles that should be just let through, we shouldn’t have to apply for funding.
Porter They need an operation.
Pailthorpe Yeah, they need an operation, it’s a barn door decision, you just need to get on and get it done sort of thing.
Merry I have paid contributions for 37 years, I can understand that good housekeeping is vital, however, when it comes to something like carpal tunnel surgery, as I understand it, when it is severe whatever you do to it at some stage surgery is going to be needed. To stop the progression of impairment in your dominant hand I would argue that any delay could be more costly to the NHS.
Porter So what happened in your case?
Merry Well what happened in my case is I have to say I made a bit of a noise. I was constantly chasing it. So when funding was approved the process was really remarkably quick. I’ve since found out there are vacant surgery slots that are not being filled with staff on standby, which is costing money, that are going vacant because they were waiting for funding requests to be approved.
Pailthorpe To me it’s almost as if some days they’ve used their quota up because it seems to be completely irrational – other ones go through without a problem and then I’ll get one rejected.
Porter What happens to those 20% of patients, what’s the risk of not operating on somebody like Ash?
Pailthorpe Well the risk in her case in fact is that the pressure on the nerve cause permanent damage.
Porter So looking at those 20% that are refused are any of them ever going to get better on their own or are they going to end up under your care having an operation at some stage?
Pailthorpe I don’t think it ever goes. The trouble is that the literature is confusing sometimes when it comes to certain treatments, particularly when it comes to simple things like carpal tunnel because sometimes there isn’t an awful lot of evidence but there’s an awful lot of common sense and experience.
Porter Because this is one of the areas that the people behind these criteria will say look there isn’t enough evidence to support this intervention and what you’re saying is it’s just because there isn’t enough evidence. It might be that the trials haven’t been done, it’s not that the procedure doesn’t work – is that what you’re saying?
Pailthorpe Yeah to a certain extent yes. Though there is, I think, more evidence coming out. There is a big study in fact in Sweden on corticosteroid injections and showed that again in certain specific instances is actually a very effective treatment and will reduce the symptoms for a year or more, though…
Porter But is it delaying the inevitable?
Pailthorpe They eventually all still come to surgery at some point because nobody has followed them up for another 10 years. And so that’s why the evidence is fundamentally flawed and I do have some patients who grumble along for years, have had some ladies who’ve come to me in their 50s, 60s and said well I’ve had it for 20 years but now actually I can’t feel my fingers. Well it’s almost too late then. So there comes a time where actually there is an opportune time to get on with it.
Porter What’s happening in other parts of the country, is this something that’s happening pretty uniformly?
Pailthorpe No I don’t think so, it seems to me that there are – some of my colleagues I’ve chatted to they say well what are IFRs – individual funding requests – they don’t have to do them. So some parts of the country it’s not active at the moment but other parts it’s obviously almost draconian.
Porter Ash mentioned empty slots where because the funding’s not coming through there’s a slot that could have been used but the team’s all still there, is that actually happening?
Pailthorpe Yes. We were planning to do a list at the end of January and we have something I think in the region of 40-50 patients where we’re waiting on funding. So it was all set to go but we just haven’t got the patients at the moment to fill the list. Overall there’s a lot of waste of money in this process. We’ve had to employ an administrative staff just for IFRs!
Porter Charles Pailthorpe and his patient Ash Merry.
Back in Cheltenham surgeon Jonothan Earnshaw treats varicose veins as well as hernias, and he too has witnessed a dramatic change in practice over recent years. His team now does half the operations it used to.
Earnshaw Over the years there’s been an increasing thought that in fact a lot of varicose veins don’t need to be done – they’re either cosmetic or there’s no medical advantage in doing them – and so we’ve had great restrictions on the sort of veins that we can treat. So we tend now only to be allowed to treat people who’ve got complications from their veins, not just simple discomfort.
Porter And the sort of complications that you’d have to have – the boxes that you’d have to tick – to get approved for your surgery would be what?
Earnshaw So if you have varicose veins long enough they start to affect the skin around your ankle and you’ve seen the brown speckling there which is called varicose eczema and that’s a sign that there’s high pressure in the veins of the skin. If you don’t treat people with varicose eczema there’s a high chance if they damage their skin they will get a varicose ulcer and varicose ulcers are common particularly in the elderly. So the idea of treating people with varicose veins is to prevent them getting the complications of varicose ulcer.
Porter And presumably once somebody develops that complication that’s expensive and difficult to deal with?
Earnshaw Oh yes and painful, it’s horrible having a varicose ulcer, it really grossly affects quality of life. And most of the guidelines and restrictions on treatment for varicose veins allow treatment of people with complicated varicose veins for that very reason. And the guidelines for varicose veins are much easier because the classification of varicose veins is easier. It’s obvious when people are starting to get complications in their veins – and those are the ones we treat – it’s obvious which are the ones don’t have complications and those generally speaking are the ones that we don’t treat.
Porter Are you happy with where the bar is set?
Earnshaw Well again the bar is very variable around the country. Here in Gloucestershire we’re allowed to treat people with complicated varicose veins and people whose varicose veins severely affect their quality of life. The problem of course is who decides whether a quality of life is severely affected and we often end up having quite uncomfortable consultations in outpatients where perhaps my perception of quality of life isn’t quite the same as the person who has their varicose veins and that can lead to considerable difficulty.
Porter So will you sometimes tell a patient in outpatients look you’re not going to meet the threshold, we’re not going to be able to operate on you or we don’t need to operate on you?
Earnshaw That happens in every clinic that I do. We have people who come with what they regard as severe symptoms from their varicose veins but actually when you question them they’re not affecting their sleep, they don’t require painkillers, they’re not actually affecting their work and under those circumstances our local commissioning wouldn’t fund that intervention. So I have to tell patients then that I can’t operate on their veins.
Porter But what happens to them if you don’t operate on their veins, I mean they’re not going to get better are they, I mean presumably with time they get worse – do they – are we just delaying the inevitable here as well?
Earnshaw Well that’s not quite the case because as a GP you’ll have had many patients who have varicose veins for years and years and years and years and years that never ever get any complications and if we could predict which people with varicose veins were going to go on and get complications then it would be easy to select those out but we can’t and most people don’t get complications from their varicose veins. So there are reasonable medicine reasons for not operating, not treating people with varicose veins, until they actually start to get the complications.
Porter So what might happen is a patient might be referred into you, you say don’t need to operate, or can’t operate now, come back when you’ve got a complication for those that do?
Earnshaw Exactly right and as a surgeon who’s been in one place for a very long time that happens not infrequently. But of course the corollary of that is that I’ve sent away a lot of people and reassured them their veins are no threat to their health and they’ve never come back over the years.
Porter Jonothan Earnshaw.
Clinical Commissioning Groups - CCGs - are in a difficult position, squeezed between the expectations of their public and the demands of their doctors and other healthcare professionals.
Buckinghamshire GP Graham Jackson is Chair of his local CCG, and co-Chair of NHS Clinical Commissioners.
Jackson Clinical Commissioning Groups are allocated a certain amount of resource from central government to spend on healthcare in their locality or their area. And what we have to do is decide how to spend that resource most effectively. Cancer services, emergency services, surgical interventions – and so we have to make decisions based on the population and remembering the populations differ from different parts of the country and then how we spend that money is based on their local need.
Porter And put simply, if you spend more money on people having minor varicose veins treated, for instance, that leaves you less money to help people who might have severe arthritis and require a hip replacement?
Jackson Well it’s certainly true there’s only a finite fixed amount of fund.
Porter One of the criticisms aimed at the current set up is that there’s something of what’s become known as the postcode lottery, that if the criteria for all of these procedures, for getting your hand surgery done, your varicose veins done or your hip done was the same in every area of the country and people understand there are limited resources then perhaps everyone would buy into it much more. Why is there this variability?
Jackson I think the variability comes back to the fact that we are locally focused and so the priorities for spending healthcare in a particular area need to be matched to the priority of that population and it’s really important to understand that the local population has different needs from different parts of the country, even actually in say the same county in different areas based on their age profile etc.
Porter And are some CCGs under more financial pressures than others because of that change in demography?
Jackson I think that is true. There is an allocation across the country from CCG to CCG based on that profile but it’s very difficult to make those allocations absolutely accurate everywhere.
Porter One of the concerns, I suppose, is that we are delaying the inevitable, so that by reducing perhaps the number of hernias that we operate on we end up maybe with more people coming in with strangulations that are expensive and obviously have implications for the patient. I presume we’re monitoring this situation ongoing to check that these interventions are cost effective in the long term?
Jackson Yes there’s a lot of monitoring going on in the number of interventions but I think it comes back to the whole picture again – we have an ageing population with an increasing number of illnesses that need to be dealt with.
Porter Do you know for sure that your gateways, if you like, to limit the treatments that are being done, to prioritise the treatments that are being done, actually work in terms of cost effectiveness, that they’re saving your CCG money?
Jackson I think there is monitoring within the system and clearly there’s a cost for those gateways and we have to be honest there is a cost to run those gateways and it’s important that those costs are monitored against the cost of procedures.
Porter Because it might be that a particular gateway that’s put in with all the best intentions might end up not working, it might not be cost effective to do that but to make that decision you need to be monitoring these very closely and that is going on is it across the country?
Jackson It is going on and then there is clearly – everything we do has a cost attached to it and the basic premise is that we have limited resource and we must not squander that resource.
Porter Yes I mean we mustn’t squander it on unnecessary treatments but we mustn’t squander it on unnecessary admin but we’re looking at the treatments from an evidence base – I mean I’m just asking are we applying those same stringent rules to the gateway interventions, to the admin behind this?
Jackson The gateway interventions are monitored monetarily but also from a quality perspective to make sure they do provide the quality assessment that we need.
Porter Dr Graham Jackson. So given that CCGs across England are monitoring the impact of prioritising treatments like hernia repairs, and hand and varicose vein surgery, we went looking for published examples of their findings. When I say we….
McCartney Mark, I may never forgive you for this. I’ve spent the last week trawling through minutes from CCGs looking to see who is looking at the harms of the procedures that people have put in place to try and limit access to interventions. I can find almost none. I can find people that have written down things like – Will this affect people, for example, older people more or carers more, qualities analysis, but I cannot find any analysis done of the cost effectiveness of the entire procedure.
Porter Well Graham says it’s being monitored, so one would imagine that if his CCG’s doing that that that’s happening across the country but what you’re saying is that nothing is being published?
McCartney I can’t find anything in the public domain, if any listeners know of any please do send it in for me. And of course there’s all sorts of other costs associated with not doing things, for example people having more physiotherapy, people attending their GP more to get painkillers, people being off work, people maybe needing to see a psychologist, people not being able to care for family or relatives. These costs, I think, are being absorbed elsewhere into the system and they’re not being properly tabulated.
Porter And of course the other aspect is the cost of the bureaucracy itself, which needs to be balanced against the cost of not doing some of these operations.
McCartney Yeah, ask GPs how much time they’re spending doing paperwork as opposed to face to face patient care – it’s huge and it’s growing and I don’t think anyone’s really got a clear handle on how much of this is being generated by CCGs and these type of rules.
Porter But we can’t be dismissive of it because we don’t know because the evidence isn’t published?
McCartney And that’s a big problem, whenever you’re putting a new policy into practice I think it should be incumbent on the policymakers to say what are the potential harms, what are the potential downsides and how are we going to find out about them because if you don’t look for them you will not find them, they will be buried and they’ll just come back to bite you on the posterior later on.
Porter Margaret McCartney – who will be one of the panellists in our upcoming hour long special debate on the NHS – what needs to give? – which will be aired on Valentine’s day. In the meantime normal service resumes next week when I will learning how virtual reality is being used to help people with conditions as diverse as Alzheimer’s disease and phantom limb pain. As well as taking a closer look at the latest initiative to limit and target antibiotic use for sore throats.
ENDSTHE ATTACHED TRANSCRIPT WAS TYPED FROM A RECORDING AND NOT COPIED FROM AN ORIGINAL SCRIPT. BECAUSE OF THE RISK OF MISHEARING AND THE DIFFICULTY IN SOME CASES OF IDENTIFYING INDIVIDUAL SPEAKERS, THE BBC CANNOT VOUCH FOR ITS COMPLETE ACCURACY.
INSIDE HEALTH
Programme 5.
TX: 31.01.17 2100-2130
PRESENTER: MARK PORTER
PRODUCER: ERIKA WRIGHT
Porter Coming up today carpal tunnel syndrome, hernias and varicose veins and why you might now struggle to get any of them treated on the NHS.
And the difficulty is not limited to these common complaints. Clinical Commissioning Groups in the Midlands have been in the headlines this week after raising the bar for eligibility for hip and knee replacements. If you live in Worcestershire your arthritis now needs to be severe enough to cause pain that interferes with daily life and keeps you awake at night. If it’s not then the local CCGs won’t pay for the surgery. A move they believe will lead to 350 fewer operations, saving them around £20 million a year to spend on other therapies they deem higher priority.
Prioritisation is otherwise known as rationing and there’s a burgeoning number of interventions on the not normally funded list, produced by CCGs to show what they are not prepared to pay for unless there are exceptional circumstances.
Clinicians with patients they regard as special cases with things like hernias have to seek approval using an individual funding request – or IFR – which is appraised by a panel to check the patient meets the necessary criteria.
Jonothan Earnshaw is Consultant Surgeon at Cheltenham General Hospital.
Earnshaw Groin hernias are very common and the danger with having a groin hernia is strangulation where a piece of bowel gets into the hernia and twists and in that circumstance people need an urgent hernia repair and sometimes even the bowel needs to be removed. And the reason for doing routine elective hernia repair is to prevent strangulation. The problem is it’s really very tricky to assess whether an individual hernia is likely to strangulate and for that reason we’ve ended up in the past operating on most people who have hernias, unless there was a strong reason not to – if someone was very elderly or unfit and very occasionally I suppose we wouldn’t treat minor, small hernias – but essentially all people with hernias had surgery for them.
Porter So fast forward to today, what’s the situation now?
Earnshaw Well over the last 10 years we’ve certainly had various different protocols that have been given to us to try and reduce the number of hernias that we operate on. Sometimes we’ve been asked to mend just painful ones or sometimes we’ve been asked mend only ones that are likely to strangulate but that’s a very non-specific way of being able to tell the difference between hernias and that’s not very helpful for me to decide whether or not to fix them.
Porter And the driver behind that has been what – the clinical evidence base that shows that some hernias don’t need treating, won’t cause trouble or is it mainly a cost issue?
Earnshaw The main driver, as with so many of these things, is cost, to reduce the number of hernias that are done that really are never going to strangulate. The science shows actually that if you take people with small hernias and there have been a couple of randomised trials where people either operate on a hernia or select patients for watchful waiting and see what happens over a number of years and if you do that over about 10 years most of the watchful waiting group get bigger and need surgery.
Porter So you might be delaying the inevitable with a lot of these patients?
Earnshaw I think that’s exactly what you’re doing.
Porter But what’s practically involved as a consultant? So I see somebody with a common type of hernia, I send them to you, you then look at them and say I think this needs an operation – what happens?
Earnshaw So at the moment the rules have changed. A couple of years ago we all had to fill a form in which was sent to the interventions not normally funded group and they checked the forms to see whether they matched criteria for surgery.
Porter So this was even though you decided that the patient needed surgery, somebody else is checking that…?
Earnshaw Was checking it, yes, and turning some of them down, saying that they weren’t suitable for repair, particularly those who had direct more mild hernias, if my clinic letter didn’t say that they had severe pain then they were often turned down.
Porter So severe pain being one of the boxes you had to tick.
Earnshaw Being one of the boxes, absolutely and in a working age person having a hernia, particularly if you’ve got a manual job, can be very uncomfortable.
Porter So are you spending a lot of your time now filling in these funding referrals for hernias?
Earnshaw No that seems to have stopped and I’ve assumed that the Clinical Commissioning Groups have found that it actually doesn’t reduce the number of people who get operations and therefore that the costs of this layer of bureaucracy actually aren’t worth it.
Porter So essentially it might have been that it was an administrative hurdle that wasn’t actually making a lot of difference.
Earnshaw Exactly right.
Porter How does your practice here compare to practices elsewhere in the country? Are you operating on a similar proportion of the hernias that you see?
Earnshaw No, my colleagues around the country tell me that there’s a very big discrepancy between who gets hernia repairs. In some places, like Gloucestershire, it’s pretty easy to get your hernia repaired if there is an appropriate reason for doing so.
Porter So that’s your decision.
Earnshaw So that’s my decision. What happens for that is that because people are able to travel is they often come over here to get their hernia repaired from neighbouring counties. In many parts of the country it’s extraordinarily difficult to get your hernia repaired and the difficulty of course is to assess which hernias are the ones which are most likely to strangulate, it’s a very difficult clinical decision.
Porter But it must be that your colleagues in other parts of the country are wanting to operate on the ones that they think might strangulate, so are they better or worse at selecting them than you or is it an inexact science?
Earnshaw It’s a very inexact science and I think it must be deeply frustrating to find that you can only operate on a very small proportion of people with hernias because hernias are uncomfortable and it’s one of the operations I do that people seem to derive most benefit from in terms of improving their symptoms.
Porter And if you’re not operating on many people you will, be default, miss some that go on to strangulate.
Earnshaw Yes and I would imagine that in areas where you don’t do a lot of elective hernia repairs you will start to see people with strangulated hernias. And fixing a strangulate hernia in an emergency is not an easy thing to do.
Porter Surgeon Jonothan Earnshaw.
Inside Health’s Margaret McCartney has been looking at what research says about the impact of limiting access to treatments like hernia surgery.
McCartney Mark, I have found the evidence, it’s taken me the best part of a week, but I can back this up. In 2009 the Department of Health had asked the management consultancy McKinsey to find out how to make services more cost effective in England and one of the things they proposed was that groin hernias in the main didn’t have to be operated on because mainly people got on just as well if they didn’t have an operation than if they did. And this was proposed as a cost saving device and as a result many CCGs decided to no longer operate routinely for people who had groin hernias that didn’t seem to be causing them much problem. And that might seem on one level absolutely fine, why interfere with something that wasn’t causing you problems anyway? But at that time no one had investigated what the consequences of this new policy would be. Well a group of surgeons went and looked to see what happened in the 16 months before and after this new policy. And what they found was that this policy change made more people who had a hernia, that hadn’t been operated on, end up turning up as an emergency, needing an emergency procedure done on that hernia that had then developed a problem.
Porter And in terms of numbers what sort of numbers are we talking about?
McCartney Overall it’s still small, so this is not to needlessly alarm people who decided on the basis of a discussion with their doctors or healthcare provider not to have surgery. But what these doctors found that was pretty much a doubling of people needing emergency repairs who hadn’t had the operation done, that was 3.6% versus 5.5%. And what was really important was the people in that group who did need emergency care tended to have more adverse effects, more problems after the surgery compared with people who’d had it done routinely. That’s the big problem.
Porter Knowing how cynical our Inside Health audience is I suppose my next question should be – well surgeons would say that wouldn’t they?
McCartney Mark, I like the cynicism, I support cynicism myself but this was just number counting, this was just looking at what happened afterwards. So I think in this study there was a limited chance of bias.
Porter So we’re looking at something like just under one in 20 people needing to have emergency surgery, if – if they were left.
McCartney Yeah, now we can’t prove cause and effect, this wasn’t a randomised control trial, it was a study looking at the association of a new policy but it’s the best data we have and that is flagging up a problem. Now it’s completely different if people are sitting down talking about what to do about a problem and making a valid decision based on individual judgement about a set of circumstances. The big problem is that McKinsey, who made the recommendation not to routinely operate on people with inguinal hernias, they based this policy on trials that were done from America, but the trials are flawed when we start to compare with them with practice in the UK of enforcing this policy because over half the people offered entry into the trials didn’t take part in it, they declined to do so, they wanted to have surgery anyway. So we cannot compare like with like, we cannot say that therefore this policy is going to benefit our patients in the UK, the data was flawed.
Porter So the findings of the research might have been skewed by the people who were included in the trial but you’re confident that this second trial, where the surgeons went to look to see what happened to these people, that that was reflective of real life practice?
McCartney Well this is real life practice, it’s not a clinical trial, we can’t prove cause and effect but we certainly can say that this policy was associated with a change in the amount of people who presented as an emergency.
Porter Margaret McCartney.
Hand surgery is another area that has been targeted by CCGs looking to save resources. Ash Merry’s specialist had to apply for funding when he felt she needed surgery for carpal tunnel syndrome – a common complaint caused by entrapment of one of the nerves supplying the hand. And it was giving her a lot of trouble.
Merry Pins and needles. Not during the day but specifically at night. And I used to lie in bed, put my hands above my head and I was kept awake literally by the pain in my right hand and it is excruciating, it’s like electric shocks going up and down your arm and you cannot stop it. It was quite literally wrecking my life I felt.
Porter And how long had that been going on before you first sought medical advice?
Merry Not sleeping at night, it has been going on intermittently probably for about a year.
Porter So you went to see your doctor?
Merry Yes. I went to see the doctor in March 2016 and I went to see a consultant before Christmas and I thought ooh this is to check yes what surgery’s going to be. No it wasn’t. We have to now apply for funding.
Porter Had you ever heard of anything like this happening before?
Merry No, I jolly well hadn’t.
Pailthorpe So I’m Charles Pailthorpe, I’m a Consultant Orthopaedic Surgeon with a specialist interest in the hand at the Royal Berkshire Hospital in Reading. My practice as a hand surgeon has changed quite dramatically over the past couple of years with the individual funding requests policy. It’s become almost an administrative nightmare, having to spend more and more time filling in forms, I don’t think it’s got any benefit to my patients at all. And the problem in hand surgery is that it affects almost half my practice, so simple, in relative terms, conditions called carpal tunnel syndrome, which is a trapped nerve, things like a trigger finger where the finger gets caught and a condition called Dupuytren’s where the finger actually gets stuck – these are common hand conditions but now have to have funding requested. CCGs have stated in their funding request information that exceptional health requirement is over and above what is there for the general public. But if you’ve got a condition that’s affecting your life and stopping you either from sleeping, like carpal tunnel syndrome or you’re unable to do your job because you can’t feel your hands and you’re dropping things why is that exceptional above the general public? It’s not and so this rationing purposes doesn’t take into effect what’s happening to the actual patient themselves.
And so from my perspective my job is to treat the patient and each patient who uses their hands is individual, we’re all individuals, we all use our hands, we all abuse our hands but we all do it differently. So what is a problem for one person isn’t for somebody else. And so actually having a checklist of so-called interventions before you can do surgery doesn’t make sense for an individual where there may well be exceptional reasons. So I’m having my professional integrity in essence questioned by having to prove exceptional health requirements.
Porter Is that part of it though, I mean that you feel that you’re being undermined professionally, I mean is that one of the reasons that I mean it gets your goat, I can feel it?
Pailthorpe You know I’ve been a hand surgeon since 1995, I think I’m not a knife happy surgeon, I’m a very cautious surgeon but when I do make a decision with the patient’s agreement that surgery’s appropriate I’d like to feel that I have the professional integrity that that’s correct.
Porter Looking at carpal tunnel syndrome, it’s a common problem, we see a lot of it in general practice, refer a lot of it to surgeons like you, how many of the patients that you feel definitely need an operation do you get approved easily or are you constantly getting refusals?
Pailthorpe We think that we’re probably getting about a 20% rejection rate and that’s largely based on a failure of the checklist concept. So if they haven’t had a splint or if they haven’t had an injection it’s often rejected, they say why haven’t they had an injection, despite the fact that I’ve put down sometimes the reason why I think an injection’s not appropriate, because there are sometimes reasons, they’ve still be rejected.
Porter Because that’s the other part of the rationalisation isn’t it, it’s not just about saving resources but it’s using resources appropriately and getting people to follow guidelines. So for instance with carpal tunnel they might get somebody like me to say we’ll try a splint for four to six weeks first, then refer to you, you might consider an injection and then surgery as a last resort.
Pailthorpe Well I don’t have a problem with that actually but there are exceptions. What we haven’t got at the moment is a way of agreeing those exceptions with the clinical groups. For example, in carpal tunnel syndrome if somebody’s got wasting of their thumb muscles that should be just let through, we shouldn’t have to apply for funding.
Porter They need an operation.
Pailthorpe Yeah, they need an operation, it’s a barn door decision, you just need to get on and get it done sort of thing.
Merry I have paid contributions for 37 years, I can understand that good housekeeping is vital, however, when it comes to something like carpal tunnel surgery, as I understand it, when it is severe whatever you do to it at some stage surgery is going to be needed. To stop the progression of impairment in your dominant hand I would argue that any delay could be more costly to the NHS.
Porter So what happened in your case?
Merry Well what happened in my case is I have to say I made a bit of a noise. I was constantly chasing it. So when funding was approved the process was really remarkably quick. I’ve since found out there are vacant surgery slots that are not being filled with staff on standby, which is costing money, that are going vacant because they were waiting for funding requests to be approved.
Pailthorpe To me it’s almost as if some days they’ve used their quota up because it seems to be completely irrational – other ones go through without a problem and then I’ll get one rejected.
Porter What happens to those 20% of patients, what’s the risk of not operating on somebody like Ash?
Pailthorpe Well the risk in her case in fact is that the pressure on the nerve cause permanent damage.
Porter So looking at those 20% that are refused are any of them ever going to get better on their own or are they going to end up under your care having an operation at some stage?
Pailthorpe I don’t think it ever goes. The trouble is that the literature is confusing sometimes when it comes to certain treatments, particularly when it comes to simple things like carpal tunnel because sometimes there isn’t an awful lot of evidence but there’s an awful lot of common sense and experience.
Porter Because this is one of the areas that the people behind these criteria will say look there isn’t enough evidence to support this intervention and what you’re saying is it’s just because there isn’t enough evidence. It might be that the trials haven’t been done, it’s not that the procedure doesn’t work – is that what you’re saying?
Pailthorpe Yeah to a certain extent yes. Though there is, I think, more evidence coming out. There is a big study in fact in Sweden on corticosteroid injections and showed that again in certain specific instances is actually a very effective treatment and will reduce the symptoms for a year or more, though…
Porter But is it delaying the inevitable?
Pailthorpe They eventually all still come to surgery at some point because nobody has followed them up for another 10 years. And so that’s why the evidence is fundamentally flawed and I do have some patients who grumble along for years, have had some ladies who’ve come to me in their 50s, 60s and said well I’ve had it for 20 years but now actually I can’t feel my fingers. Well it’s almost too late then. So there comes a time where actually there is an opportune time to get on with it.
Porter What’s happening in other parts of the country, is this something that’s happening pretty uniformly?
Pailthorpe No I don’t think so, it seems to me that there are – some of my colleagues I’ve chatted to they say well what are IFRs – individual funding requests – they don’t have to do them. So some parts of the country it’s not active at the moment but other parts it’s obviously almost draconian.
Porter Ash mentioned empty slots where because the funding’s not coming through there’s a slot that could have been used but the team’s all still there, is that actually happening?
Pailthorpe Yes. We were planning to do a list at the end of January and we have something I think in the region of 40-50 patients where we’re waiting on funding. So it was all set to go but we just haven’t got the patients at the moment to fill the list. Overall there’s a lot of waste of money in this process. We’ve had to employ an administrative staff just for IFRs!
Porter Charles Pailthorpe and his patient Ash Merry.
Back in Cheltenham surgeon Jonothan Earnshaw treats varicose veins as well as hernias, and he too has witnessed a dramatic change in practice over recent years. His team now does half the operations it used to.
Earnshaw Over the years there’s been an increasing thought that in fact a lot of varicose veins don’t need to be done – they’re either cosmetic or there’s no medical advantage in doing them – and so we’ve had great restrictions on the sort of veins that we can treat. So we tend now only to be allowed to treat people who’ve got complications from their veins, not just simple discomfort.
Porter And the sort of complications that you’d have to have – the boxes that you’d have to tick – to get approved for your surgery would be what?
Earnshaw So if you have varicose veins long enough they start to affect the skin around your ankle and you’ve seen the brown speckling there which is called varicose eczema and that’s a sign that there’s high pressure in the veins of the skin. If you don’t treat people with varicose eczema there’s a high chance if they damage their skin they will get a varicose ulcer and varicose ulcers are common particularly in the elderly. So the idea of treating people with varicose veins is to prevent them getting the complications of varicose ulcer.
Porter And presumably once somebody develops that complication that’s expensive and difficult to deal with?
Earnshaw Oh yes and painful, it’s horrible having a varicose ulcer, it really grossly affects quality of life. And most of the guidelines and restrictions on treatment for varicose veins allow treatment of people with complicated varicose veins for that very reason. And the guidelines for varicose veins are much easier because the classification of varicose veins is easier. It’s obvious when people are starting to get complications in their veins – and those are the ones we treat – it’s obvious which are the ones don’t have complications and those generally speaking are the ones that we don’t treat.
Porter Are you happy with where the bar is set?
Earnshaw Well again the bar is very variable around the country. Here in Gloucestershire we’re allowed to treat people with complicated varicose veins and people whose varicose veins severely affect their quality of life. The problem of course is who decides whether a quality of life is severely affected and we often end up having quite uncomfortable consultations in outpatients where perhaps my perception of quality of life isn’t quite the same as the person who has their varicose veins and that can lead to considerable difficulty.
Porter So will you sometimes tell a patient in outpatients look you’re not going to meet the threshold, we’re not going to be able to operate on you or we don’t need to operate on you?
Earnshaw That happens in every clinic that I do. We have people who come with what they regard as severe symptoms from their varicose veins but actually when you question them they’re not affecting their sleep, they don’t require painkillers, they’re not actually affecting their work and under those circumstances our local commissioning wouldn’t fund that intervention. So I have to tell patients then that I can’t operate on their veins.
Porter But what happens to them if you don’t operate on their veins, I mean they’re not going to get better are they, I mean presumably with time they get worse – do they – are we just delaying the inevitable here as well?
Earnshaw Well that’s not quite the case because as a GP you’ll have had many patients who have varicose veins for years and years and years and years and years that never ever get any complications and if we could predict which people with varicose veins were going to go on and get complications then it would be easy to select those out but we can’t and most people don’t get complications from their varicose veins. So there are reasonable medicine reasons for not operating, not treating people with varicose veins, until they actually start to get the complications.
Porter So what might happen is a patient might be referred into you, you say don’t need to operate, or can’t operate now, come back when you’ve got a complication for those that do?
Earnshaw Exactly right and as a surgeon who’s been in one place for a very long time that happens not infrequently. But of course the corollary of that is that I’ve sent away a lot of people and reassured them their veins are no threat to their health and they’ve never come back over the years.
Porter Jonothan Earnshaw.
Clinical Commissioning Groups - CCGs - are in a difficult position, squeezed between the expectations of their public and the demands of their doctors and other healthcare professionals.
Buckinghamshire GP Graham Jackson is Chair of his local CCG, and co-Chair of NHS Clinical Commissioners.
Jackson Clinical Commissioning Groups are allocated a certain amount of resource from central government to spend on healthcare in their locality or their area. And what we have to do is decide how to spend that resource most effectively. Cancer services, emergency services, surgical interventions – and so we have to make decisions based on the population and remembering the populations differ from different parts of the country and then how we spend that money is based on their local need.
Porter And put simply, if you spend more money on people having minor varicose veins treated, for instance, that leaves you less money to help people who might have severe arthritis and require a hip replacement?
Jackson Well it’s certainly true there’s only a finite fixed amount of fund.
Porter One of the criticisms aimed at the current set up is that there’s something of what’s become known as the postcode lottery, that if the criteria for all of these procedures, for getting your hand surgery done, your varicose veins done or your hip done was the same in every area of the country and people understand there are limited resources then perhaps everyone would buy into it much more. Why is there this variability?
Jackson I think the variability comes back to the fact that we are locally focused and so the priorities for spending healthcare in a particular area need to be matched to the priority of that population and it’s really important to understand that the local population has different needs from different parts of the country, even actually in say the same county in different areas based on their age profile etc.
Porter And are some CCGs under more financial pressures than others because of that change in demography?
Jackson I think that is true. There is an allocation across the country from CCG to CCG based on that profile but it’s very difficult to make those allocations absolutely accurate everywhere.
Porter One of the concerns, I suppose, is that we are delaying the inevitable, so that by reducing perhaps the number of hernias that we operate on we end up maybe with more people coming in with strangulations that are expensive and obviously have implications for the patient. I presume we’re monitoring this situation ongoing to check that these interventions are cost effective in the long term?
Jackson Yes there’s a lot of monitoring going on in the number of interventions but I think it comes back to the whole picture again – we have an ageing population with an increasing number of illnesses that need to be dealt with.
Porter Do you know for sure that your gateways, if you like, to limit the treatments that are being done, to prioritise the treatments that are being done, actually work in terms of cost effectiveness, that they’re saving your CCG money?
Jackson I think there is monitoring within the system and clearly there’s a cost for those gateways and we have to be honest there is a cost to run those gateways and it’s important that those costs are monitored against the cost of procedures.
Porter Because it might be that a particular gateway that’s put in with all the best intentions might end up not working, it might not be cost effective to do that but to make that decision you need to be monitoring these very closely and that is going on is it across the country?
Jackson It is going on and then there is clearly – everything we do has a cost attached to it and the basic premise is that we have limited resource and we must not squander that resource.
Porter Yes I mean we mustn’t squander it on unnecessary treatments but we mustn’t squander it on unnecessary admin but we’re looking at the treatments from an evidence base – I mean I’m just asking are we applying those same stringent rules to the gateway interventions, to the admin behind this?
Jackson The gateway interventions are monitored monetarily but also from a quality perspective to make sure they do provide the quality assessment that we need.
Porter Dr Graham Jackson. So given that CCGs across England are monitoring the impact of prioritising treatments like hernia repairs, and hand and varicose vein surgery, we went looking for published examples of their findings. When I say we….
McCartney Mark, I may never forgive you for this. I’ve spent the last week trawling through minutes from CCGs looking to see who is looking at the harms of the procedures that people have put in place to try and limit access to interventions. I can find almost none. I can find people that have written down things like – Will this affect people, for example, older people more or carers more, qualities analysis, but I cannot find any analysis done of the cost effectiveness of the entire procedure.
Porter Well Graham says it’s being monitored, so one would imagine that if his CCG’s doing that that that’s happening across the country but what you’re saying is that nothing is being published?
McCartney I can’t find anything in the public domain, if any listeners know of any please do send it in for me. And of course there’s all sorts of other costs associated with not doing things, for example people having more physiotherapy, people attending their GP more to get painkillers, people being off work, people maybe needing to see a psychologist, people not being able to care for family or relatives. These costs, I think, are being absorbed elsewhere into the system and they’re not being properly tabulated.
Porter And of course the other aspect is the cost of the bureaucracy itself, which needs to be balanced against the cost of not doing some of these operations.
McCartney Yeah, ask GPs how much time they’re spending doing paperwork as opposed to face to face patient care – it’s huge and it’s growing and I don’t think anyone’s really got a clear handle on how much of this is being generated by CCGs and these type of rules.
Porter But we can’t be dismissive of it because we don’t know because the evidence isn’t published?
McCartney And that’s a big problem, whenever you’re putting a new policy into practice I think it should be incumbent on the policymakers to say what are the potential harms, what are the potential downsides and how are we going to find out about them because if you don’t look for them you will not find them, they will be buried and they’ll just come back to bite you on the posterior later on.
Porter Margaret McCartney – who will be one of the panellists in our upcoming hour long special debate on the NHS – what needs to give? – which will be aired on Valentine’s day. In the meantime normal service resumes next week when I will learning how virtual reality is being used to help people with conditions as diverse as Alzheimer’s disease and phantom limb pain. As well as taking a closer look at the latest initiative to limit and target antibiotic use for sore throats.
ENDS |
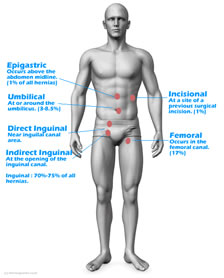

Site / Currency Conversion Customer Services Business Address
© 2024 Blueray Pharma Ltd Registered in England Company No. 9124059 |












